
Tips on How to Write a Euthanasia Argumentative Essay

Abortion, birth control, death sentencing, legalization of medical marijuana, and gender reassignment surgery remain the most controversial medical issues in contemporary society. Euthanasia is also among the controversial topics in the medical field. It draws arguments from philosophy, ethics, and religious points of view.
By definition derives from a Greek term that means good death, and it is the practice where an experienced medical practitioner or a physician intentionally ends an individual's life to end pain and suffering. The names mercy killing or physician-assisted suicide also knows it.
Different countries have different laws as regards euthanasia. In the UK, physician-assisted suicide is illegal and can earn a medical practitioner 14 years imprisonment. All over the world, there is a fierce debate as regards mercy killing.
Like any other controversial topic, there are arguments for and against euthanasia. Thus, there are two sides to the debate. The proponents or those for euthanasia believe it is a personal choice issue, even when death is involved.
On the other hand, those against euthanasia or the opponents believe that physicians must only assist patients when the patients are sound to make such a decision. That is where the debate centers.
This article explores some of the important basics to follow when writing an exposition, argumentative, persuasive, or informative essay on euthanasia.
Steps in Writing a Paper on Euthanasia
When assigned homework on writing a research paper or essay on euthanasia, follow these steps to make it perfect.
1. Read the Prompt
The essay or research paper prompt always have instructions to follow when writing any academic work. Students, therefore, should read it to pick up the mind of the professor or teaching assistant on the assigned academic task. When reading the prompt, be keen to understand what approach the professor prefers. Besides, it should also tell you the type of essay you are required to write and the scope.
2. Choose a Captivating Topic
After reading the prompt, you are required to frame your euthanasia essay title. Make sure that the title you choose is captivating enough as it invites the audience to read your essay. The title of your essay must not divert from the topic, but make it catchy enough to lure and keep readers. An original and well-structured essay title on euthanasia should give an idea of what to expect in the body paragraphs. It simply gives them a reason to read your essay.
3. Decide on the Best Thesis Statement for your Euthanasia Essay
Creating a thesis statement for a euthanasia essay does not deviate from the conventions of essay writing. The same is consistent when writing a thesis statement for a euthanasia research paper. The thesis statement can be a sentence or two at the end of the introduction that sums up your stance on the topic of euthanasia. It should be brief, well crafted, straight to the point, and outstanding. Right from the start, it should flow with the rest of the essay and each preceding paragraph should support the thesis statement.
4. Write an Outline
An outline gives you a roadmap of what to write in each part of the essay, including the essay hook, introduction, thesis statement, body paragraphs, and the conclusion. We have provided a sample euthanasia essay outline in this article, be sure to look at it.
5. Write the First Draft
With all ingredients in place, it is now time to write your euthanasia essay by piecing up all the different parts. Begin with an essay hook, then the background information on the topic, then the thesis statement in the introduction. The body paragraphs should each contain an idea that is well supported with facts from books, journals, articles, and other scholarly sources. Be sure to follow the MLA, APA, Harvard, or Chicago formatting conventions when writing the paper as advised in the essay prompt.
6. Proofread and Edit the Essay
You have succeeded in skinning the elephant, and it is now time to cut the pieces and consume. Failure to proofread and edit an essay can be dangerous for your grade. There is always an illusion that you wrote it well after all. However, if you take some time off and come to it later, you will notice some mistakes. If you want somebody to proofread your euthanasia essay, you can use our essay editing service . All the same, proofreading an essay is necessary before turning the essay in.
Creating a Euthanasia Essay or Research Paper Outline
Like any other academic paper, having a blueprint of the entire essay on euthanasia makes it easy to write. Writing an outline is preceded by choosing a great topic. In your outline or structure of argumentative essay on euthanasia, you should highlight the main ideas such as the thesis statement, essay hook, introduction, topic sentences for the body paragraphs and supporting facts, and the concluding remarks. Here is a sample outline for a euthanasia argumentative essay.
This is a skeleton for your euthanasia essay:
Introduction
- Hook sentence/ attention grabber
- Thesis statement
- Background statement (history of euthanasia and definition)
- Transition to Main Body
- The legal landscape of euthanasia globally
- How euthanasia affects physician-patient relationships
- Biblical stance on euthanasia
- Consequences of illegal euthanasia
- Ethical and moral issues of euthanasia
- Philosophical stance on euthanasia
- Transition to Conclusion
- Restated thesis statement
- Unexpected twist or a final argument
- Food for thought
Sample Euthanasia Essay Outline
Title: Euthanasia is not justified
Essay hook - It is there on TV, but did you know that a situation could prompt a doctor to bring to an end suffering and pain to a terminally ill patient? There is more than meets the eye on euthanasia.
Thesis statement : despite the arguments for and against euthanasia, it is legally and morally wrong to kill any person, as it is disregard of the right to life of an individual and the value of human life.
Paragraph 1: Euthanasia should be condemned as it ends the sacred lives of human beings.
- Only God gives life and has the authority to take it and not humans.
- The bible says, Thou shalt not kill.
- The Quran states, "Whoever killed a Mujahid (a person who is granted the pledge of protection by the Muslims) shall not smell the fragrance of Paradise though its fragrance can be smelt at a distance of forty years (of traveling).
Paragraph 2: Euthanasia gives physicians the power to determine who lives and who dies.
- Doctors end up playing the role of God.
- It could be worse when doctors make mistakes or advance their self-interests to make money. They can liaise with family members to kill for the execution of a will.
Paragraph 3: it destroys the patient-physician relationship
- Patients trust the doctors for healing
- When performed on other patients, the remaining patients lose trust in the same doctor of the facility.
- Under the Hippocratic Oath, doctors are supposed to alleviate pain, end suffering, and protect life, not eliminate it.
Paragraph 4: euthanasia is a form of murder
- Life is lost in the end.
- There are chances that when tried with other therapeutic and non-therapeutic approaches, terminally ill patients can always get better.
- It is selfish to kill a patient based on a medical report, which in itself could be erratic.
- Patients respond well to advanced care approaches.
Paragraph 5: ( Counterargument) euthanasia proponents argue based on relieving suffering and pain as well as reducing the escalating cost of healthcare.
- Euthanasia helps families avoid spending much on treating a patient who might not get well.
- It is the wish of the patients who have made peace with the fact that they might not recover.
Conclusion
In sum, advancement in technology in the medical field and the existence of palliative care are evidence enough that there is no need for mercy killing. Even though there are claims that it ends pain and suffering, it involves killing a patient who maybe could respond to novel approaches to treatment.
Abohaimed, S., Matar, B., Al-Shimali, H., Al-Thalji, K., Al-Othman, O., Zurba, Y., & Shah, N. (2019). Attitudes of Physicians towards Different Types of Euthanasia in Kuwait. Medical Principles and Practice , 28 (3), 199-207.
Attell, B. K. (2017). Changing attitudes toward euthanasia and suicide for terminally ill persons, 1977 to 2016: an age-period-cohort analysis. OMEGA-Journal of Death and Dying , 0030222817729612.
Barone, S., & Unguru, Y. (2017). Should Euthanasia Be Considered Iatrogenic? AMA journal of ethics, 19(8), 802-814.
Emanuel, E. (2017). Euthanasia and physician-assisted suicide: focus on the data. The Medical Journal of Australia , 206 (8), 1-2e1.
Inbadas, H., Zaman, S., Whitelaw, S., & Clark, D. (2017). Declarations on euthanasia and assisted dying. Death Studies, 41 (9), 574-584.
Jacobs, R. K., & Hendricks, M. (2018). Medical students' perspectives on euthanasia and physician-assisted suicide and their views on legalising these practices in South Africa. South African Medical Journal , 108 (6), 484-489.
Math, S. B., & Chaturvedi, S. K. (2012). Euthanasia: the right to life vs right to die. The Indian journal of medical research, 136 (6), 899.
Reichlin, M. (2001). Euthanasia in the Netherlands. KOS , (193), 22-29.
Saul, H. (2014, November 5). The Vatican Condemns Brittany Maynard's Decision to end her Life as �Absurd'.
Sulmasy, D. P., Travaline, J. M., & Louise, M. A. (2016). Non-faith-based arguments against physician-assisted suicide and euthanasia. The Linacre Quarterly, 83 (3), 246-257.
Euthanasia Essay Introduction Ideas
An introduction is a gate into the compound of your well-reasoned thoughts, ideas, and opinions in an essay. As such, the introduction should be well structured in a manner that catches the attention of the readers from the onset.
While it seems the hardest thing to do, writing an introduction should never give you the fear of stress, blank page, or induce a writer's block. Instead, it should flow right from the essay hook to the thesis statement.
Given that you can access statistics, legal variations, and individual stories based on personal experiences with euthanasia online, writing a euthanasia essay introduction should be a walk in the park.
Ensure that the introduction to the essay is catchy, appealing, and informative. Here are some ideas to use:
- Rights of humans to life
- How euthanasia is carried out
- When euthanasia is legally allowed
- Stories from those with experience in euthanasia
- The stance of doctors on euthanasia
- Definition of euthanasia
- Countries that allow euthanasia
- Statistics of physicians assisted suicide in a given state, locality, or continent.
- Perception of the public given the diversity of culture
There are tons of ideas on how to start an essay on euthanasia. You need to research, immerse yourself in the topic, and scoop the best evidence. Presenting facts in an argumentative essay on euthanasia will help convince the readers to argue for or against euthanasia. Based on your stance, make statements in favor of euthanasia or statements against euthanasia known from the onset through the strong thesis statement.
Essay Topics and Ideas on Euthanasia
- Should Euthanasia be legal?
- What are the different types of euthanasia?
- Is euthanasia morally justified?
- Cross-cultural comparison of attitudes and beliefs on euthanasia
- The history of euthanasia
- Euthanasia from a Patient's Point of View
- Should euthanasia be considered Iatrogenic?
- Does euthanasia epitomize failed medical approaches?
- How does euthanasia work?
- Should Physician-Assisted Suicide be legal?
- Sociology of Death and Dying
- Arguments for and against euthanasia and assisted suicide
- Euthanasia is a moral dilemma
- The euthanasia debate
- It Is Much Better to Die with Dignity Than to Live with Pain Essay
- Euthanasia Is a Moral, Ethical, and Proper
- Euthanasia Law of Euthanasia in California and New York
- Effect of Euthanasia on Special Population
- Euthanasia is inhuman
- Role of nurses in Euthanasia
- Are family and relative decisions considered during the euthanasia
- The biblical stance on euthanasia
Related Articles:
- Argumentative essay topics and Ideas
- Topics and ideas for informative essays
Get Help with Writing Euthanasia Argumentative Essay for School
We have covered the tips of writing an argumentative essay on euthanasia. Besides, we have also presented a sample euthanasia essay outline, which can help you write your essay. However, sometimes you might lack the motivation to write an essay on euthanasia, even when you have access to argumentative essay examples on euthanasia.
It is the right time to pay someone to write your argumentative essay . We have the best essay writers who have expertise in creating the best argumentative essays on any topic. They understand the entire process of argumentative writing and can create a top-grade euthanasia essay within the shortest turnaround time.
Do not wait until it is too late; let our nerds help you ace your homework. Order an essay today and forget your academic writing woes.
Order Essay on Euthanasia!
Gradecrest is a professional writing service that provides original model papers. We offer personalized services along with research materials for assistance purposes only. All the materials from our website should be used with proper references. See our Terms of Use Page for proper details.
- Type 2 Diabetes
- Heart Disease
- Digestive Health
- Multiple Sclerosis
- COVID-19 Vaccines
- Occupational Therapy
- Healthy Aging
- Health Insurance
- Public Health
- Patient Rights
- Caregivers & Loved Ones
- End of Life Concerns
- Health News
- Thyroid Test Analyzer
- Doctor Discussion Guides
- Hemoglobin A1c Test Analyzer
- Lipid Test Analyzer
- Complete Blood Count (CBC) Analyzer
- What to Buy
- Editorial Process
- Meet Our Medical Expert Board
Arguments in Favor of Right-to-Die Legislation
There are many arguments about whether people should have the right to die when they choose, intentionally and by design, to end their own perceived pain and suffering .
Differences of Opinion
Most of the arguments for and against the right to die are ideological, based on many important aspects of civility: the law, religion or spiritual beliefs, ethics, and social mores. Opinions vary based on personal experiences, belief systems, age, culture, and other aspects of humankind that influence how we think about important aspects of life.
Where the Right to Die Is Legal
In the United States, with the exception of a small number of states which have passed right-to-die legislation, a doctor who injects a patient who wants to die with a lethal drug and kills him would technically have committed murder. Proponents of right-to-die legislation desire a legal remedy for doctors who assist their suffering patients in ending their lives. Outside of the United States, euthanasia is the law of the land in Canada, the Netherlands, Colombia, Belgium, Luxembourg, and Switzerland.
Understanding Right-to-Die Laws
Right-to-Die legislation, also known as physician-assisted death or aid in dying, gives mentally competent adult patients with a terminal illness and a prognosis of six months or less to have the ability to request and receive a prescription medication to bring about their death. Most statutes under consideration at the state level are modeled after Oregon’s Death with Dignity Act, which requires two physicians to confirm the patient’s residence, diagnosis, prognosis, mental competence, and voluntariness of the request to die. In addition, two waiting periods are required.
The Pros for Right-to-Die Laws
Here are some arguments in favor of giving patients the right to die and protecting healthcare providers who carry out those wishes. Compare these arguments in favor of death with dignity and the right to die against the cons .
- A patient's death brings him or her the end of pain and suffering.
- Patients have an opportunity to die with dignity, without fear that they will lose their physical or mental capacities.
- The overall healthcare financial burden on the family is reduced.
- Patients can arrange for final goodbyes with loved ones.
- If planned for in advance, organs can be harvested and donated .
- With physician assistance , patients have a better chance of experiencing a painless and less traumatic death (death with dignity).
- Patients can end pain and suffering when there is no hope for relief.
- Some say assisted death with dignity is against the Hippocratic Oath; however, the statement “first do no harm” can also apply to helping a patient find the ultimate relief from pain through death.
- Medical advances have enabled life beyond what nature might have allowed, but that is not always in the best interest of the suffering patient with no hope of recovery.
- A living will, considered a guiding document for a patient's healthcare wishes, can provide clear evidence of a patient's decisions regarding end-of-life care.
Pereira J. Legalizing euthanasia or assisted suicide: the illusion of safeguards and controls . Curr Oncol . 2011;18(2):e38-45. doi:10.3747/co.v18i2.883
Battin MP, Van der heide A, Ganzini L, Van der wal G, Onwuteaka-philipsen BD. Legal physician-assisted dying in Oregon and the Netherlands: evidence concerning the impact on patients in "vulnerable" groups . J Med Ethics . 2007;33(10):591-7. doi:10.1136/jme.2007.022335
By Trisha Torrey Trisha Torrey is a patient empowerment and advocacy consultant. She has written several books about patient advocacy and how to best navigate the healthcare system.
Home — Essay Samples — Social Issues — Euthanasia — Why Euthanasia Should Be Legal: Analysis of Arguments and Counterarguments
Why Euthanasia Should Be Legal: Analysis of Arguments and Counterarguments
- Categories: Assisted Suicide Euthanasia Right to Die
About this sample

Words: 1865 |
10 min read
Published: Aug 14, 2023
Words: 1865 | Pages: 4 | 10 min read
Table of contents
Introduction, why euthanasia should be legal, works cited, counterarguments.
- Corder, Mike. “Dutch Euthanasia Center Sees 22% Rise in Requests in 2019.” WAVY.com, 7 Feb. 2020, www.wavy.com/news/health/dutch-euthanasia-center-sees-22-rise-in-requests-in-2019/. Accessed 10 March 2020.
- Davis, Jacky. “Kevin Davis Deserved Choice.” Dignity in Dying, www.dignityindying.org.uk/story/kevin-davis/. Accessed 13 March 2020.
- De La Torre, Esther B. The Right to Assisted Suicide, www.lonestar.edu/rightto-assist-suicide.htm. Accessed 19 March 2020.
- “Euthanasia Laws - Information on the Law about Euthanasia.” Information on the Law about Euthanasia - Suicide, Life, Act, and Mercy - JRank Articles, law.jrank.org/pages/11858/Euthanasia.html. Accessed 10 March 2020.

Cite this Essay
Let us write you an essay from scratch
- 450+ experts on 30 subjects ready to help
- Custom essay delivered in as few as 3 hours
Get high-quality help

Dr Jacklynne
Verified writer
- Expert in: Social Issues

+ 120 experts online
By clicking “Check Writers’ Offers”, you agree to our terms of service and privacy policy . We’ll occasionally send you promo and account related email
No need to pay just yet!
Related Essays
1 pages / 670 words
3 pages / 1552 words
2 pages / 1011 words
1 pages / 484 words
Remember! This is just a sample.
You can get your custom paper by one of our expert writers.
121 writers online
Still can’t find what you need?
Browse our vast selection of original essay samples, each expertly formatted and styled
Related Essays on Euthanasia
The debate surrounding euthanasia is complex and multifaceted, involving considerations of ethics, religion, personal autonomy, and the value of human life. While advocates argue that euthanasia provides relief to those [...]
Darren, Sweeper. "Euthanasia - Pros and Cons of Mercy Killing." (n.d.). 2010. Web. "Definition of Euthanasia." 1998. Web. Fletcher, Joseph. "The Courts and Euthanasia." Law, Medicine & Health Care 15.4 (1987/1988): 223-230. [...]
The topic of euthanasia, the deliberate termination of a person's life to end their suffering, has ignited ethical debates worldwide. The arguments surrounding euthanasia often involve deductive reasoning to support positions [...]
Euthanasia is the act of intentionally ending a life to relieve pain and suffering. It is a controversial topic that has been debated for centuries due to its ethical, legal, and social implications. This essay will provide an [...]
Battin, M. P., Rhodes, R., & Silvers, A. (2015). The Patient as Victim and Vector: Can Ethics Abandon the Ideal of the Autonomous Patient? The American Journal of Bioethics, 15(3), 3-14.Pereira, J. M. (2011). Legalizing [...]
Imagine facing a terminal illness with no hope for recovery, only prolonged suffering and pain. In such situations, the concept of euthanasia, or assisted suicide, becomes a controversial but increasingly relevant topic. [...]
Related Topics
By clicking “Send”, you agree to our Terms of service and Privacy statement . We will occasionally send you account related emails.
Where do you want us to send this sample?
By clicking “Continue”, you agree to our terms of service and privacy policy.
Be careful. This essay is not unique
This essay was donated by a student and is likely to have been used and submitted before
Download this Sample
Free samples may contain mistakes and not unique parts
Sorry, we could not paraphrase this essay. Our professional writers can rewrite it and get you a unique paper.
Please check your inbox.
We can write you a custom essay that will follow your exact instructions and meet the deadlines. Let's fix your grades together!
Get Your Personalized Essay in 3 Hours or Less!
We use cookies to personalyze your web-site experience. By continuing we’ll assume you board with our cookie policy .
- Instructions Followed To The Letter
- Deadlines Met At Every Stage
- Unique And Plagiarism Free

The Ethics of Euthanasia
Malleeka Suy | SQ Blogger | SQ Online (2021-2022)
Picture t his: It is the year 3020, and the Martian soil you have been drilling into has finally worked out. Colonizing Mars is taking shape, and soon your family can permanently live on this rusty, rocky planet. However, the effects of progress don’t go unnoticed; every time you move, your skin screams in pain. Everything you once loved doing has lost its appeal. Would you take death in your own hands or live until a painful end?
This moral dilemma seems straight out of a science-fiction novel for most, but euthanasia is a legitimate deliberation for patients with terminal and mental illnesses who deem their lives too painful to live on. It is a practice that is still heavily debated in modern bioethics. Among many definitions, the American Medical Association defines euthanasia as the administration of a lethal agent by a medical professional to a patient to relieve their intolerable or incurable suffering.
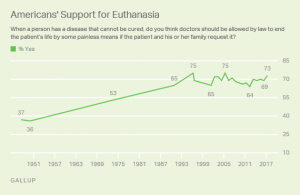
Although euthanasia is not a new scientific process, as it has been practiced since the time of the ancient Greeks more than three thousand years ago, it wasn’t generally accepted by Western medicine until recently. The Netherlands was the first country to allow legal euthanasia and assisted suicide in 2002, totaling 1.7-2.8% of total deaths. Euthanasia is generally illegal in the United States, but in a nationwide 2017 American poll , 73% of the public were in favor of euthanasia, and 57% said euthanasia is morally acceptable. These numbers are nearly double the initial poll in 1947. If I had to guess why, it may be partly because of progressive exposure to mental health and its effects. This may have allowed people to understand and empathize with the circumstances and support what euthanasia stands for: a release from an unbearable life.
Euthanasia is especially controversial among general society and the bioethical community. One main argument for the support of euthanasia is grounded in personal autonomy–our ability to act independently– since living life is about minimizing physical pain and maximizing dignity and control . This idea is rooted in ancient times when physicians considered dying with peace and dignity a human right. An article from Stanford’s Encyclopedia of Philosophy regards autonomy as self-determination, so choices about how and when people die is them taking responsibility for their lives. Terminally ill patients in Oregon mentioned how they chose euthanasia because their condition stripped them of their independence and ability to engage in activities that gave their life meaning. After all, what is the meaning of life if we cannot live it?
Another article by the Linacre Quarterly highlights how the ethics of compassion justify the use of euthanasia. From a humanitarian standpoint, we can show compassion by suffering and sympathizing with patients and respecting their wishes of euthanasia as their “remedy.” Kenneth L. Vaux, a consultant in medical ethics, notes in his article that physicians would give a lethal dose to their loved ones out of love if they were dying and suffering, so he finds it “strange and hypocritical” that doctors cannot legally do so for their patients. He claims that “we have lost empathy, sympathy, and the covenant of care with those who have entrusted their lives to us because they believe we embody those very qualities.” Vaux also asks: “Having barred the door to Death, are we not then obliged at some point to open it?” He suggests that since doctors bring life into the world every day, consensually ending a patient’s life for their benefit should be no different.
Despite popular social support, there are many arguments against euthanasia as well–the most popular being religion. Several faiths, such as Christianity, see euthanasia as a form of murder and find it to be morally unacceptable because it may weaken society’s respect for the sanctity of life. Religious groups actively argue against euthanasia, and for this reason, euthanasia became a debate of preservation and purity of life.
Even though medicine is rooted in science, some physicians also use religion as justification against practicing euthanasia. Contrary to public British opinion, studies show that most UK doctors do not support legislation permitting euthanasia due to their religiosity or faith, and less than a quarter of doctors would be willing to practice euthanasia if it became legal.
Physicians also have a professional obligation to fulfill that becomes morally blurred with euthanasia. For more than 2,500 years, doctors have taken the Hippocratic Oath to do no harm and treat those under their care. Does bringing death by euthanasia violate the Hippocratic Oath, or is it in line with a doctor’s mission? Would acting under Hippocrates then make a doctor a hypocrite?
Because of this subjectivity, doctors sometimes feel uncertain about administering euthanasia. Even if a patient is under a lot of pain and medication, how can doctors be sure that their decision was made rationally? In a Dutch article , an experienced psychiatrist dealing with a patient’s invisible suffering made him uncertain about assessing how deeply rooted their suffering really was, and therefore how moral it would be to allow euthanasia to happen. The fickle nature of the human mind makes many physicians and ethicists question whether or not euthanasia should be a normal practice.
Physicians often have their own reservations about euthanasia and how they cope with patients who wish for it. They frequently feel pressured by the patient or the patient’s relatives to perform euthanasia. A 2011 survey among Dutch physicians also found that 86% of physicians dread the emotional burden of performing euthanasia. One physician recounts how a patient told them, “If you won’t perform euthanasia, I might go to a railway line or climb a high building.” This form of blackmail can lead to dangerous expectations, where future normativity of the practice is anticipated or even praised.
Instead of placing the burden on doctors, what if the government or even robots could control euthanasia? Although this faceless jurisdiction seems like a good solution, critics argue that euthanasia would be normalized and twisted for eugenic purposes, adding to the nightmare of AI domination and impeding the sanctity and preciousness of life. These speculations seem inconceivable, but history has unfortunately seen it happen, such as in Hitler’s Germany, where Aktion T4, a Euthanasia Program systematically murdered patients with disabilities to restore the “integrity” of the German nation, thrived. Perhaps then a grimmer alternative to the use of euthanasia is the elimination of incurable, disabled, or elderly patients. Mechanization of euthanasia would also impact the patient and the medical profession, both in what it means to be human and obeying the Hippocratic Oath. Routinization of the practice could also increase the desires of people’s wishes to end their lives, whether individually justified or not.
References:
https://jamanetwork.com/journals/jama/article-abstract/2532018
https://plato.stanford.edu/entries/euthanasia-voluntary/#MoraCaseForVoluEuth
http://www.cirugiaycirujanos.com/frame_esp.php?id=308
https://www.sciencedirect.com/science/article/pii/S0885392414003066?via%3Dihub
https://www.healthline.com/health/what-is-euthanasia#making-a-decision
https://livinganddyingwell.org.uk/wp-content/uploads/2020/02/Redefining-Physicians-Role-in-Assisted-Dying.pdf
https://shibbolethsp.jstor.org/start?entityID=urn%3Amace%3Aincommon%3Aucsd.edu&dest=
https://www.jstor.org/stable/3561966&site=jstor
https://doi.org/10.1177%2F0269216310397688
https://www.medicalnewstoday.com/articles/182951#some-statistics
https://journals.sagepub.com/doi/10.1177/0269216310397688
https://www.nejm.org/doi/10.1056/NEJMclde1310667
https://medicine.missouri.edu/centers-institutes-labs/health-ethics/faq/euthanasia
https://news.gallup.com/poll/211928/majority-americans-remain-supportive-euthanasia.aspx
https://www.ama-assn.org/delivering-care/ethics/euthanasia
https://pubmed.ncbi.nlm.nih.gov/21145197/
https://doi.org/10.1016/j.jpainsymman.2014.04.016
https://www.ccsenet.org/journal/index.php/gjhs/article/view/19405/13366
https://encyclopedia.ushmm.org/content/en/article/euthanasia-program
- - Google Chrome
Intended for healthcare professionals
- Access provided by Google Indexer
- My email alerts
- BMA member login
- Username * Password * Forgot your log in details? Need to activate BMA Member Log In Log in via OpenAthens Log in via your institution
Search form
- Advanced search
- Search responses
- Search blogs
- News & Views
- Euthanasia and...
Euthanasia and assisted dying: the illusion of autonomy—an essay by Ole Hartling
Read our coverage of the assisted dying debate.
- Related content
- Peer review
- Ole Hartling , former chairman
- Danish Council of Ethics, Denmark
- hartling{at}dadlnet.dk
As a medical doctor I have, with some worry, followed the assisted dying debate that regularly hits headlines in many parts of the world. The main arguments for legalisation are respecting self-determination and alleviating suffering. Since those arguments appear self-evident, my book Euthanasia and the Ethics of a Doctor’s Decisions—An Argument Against Assisted Dying 1 aimed to contribute to the international debate on this matter.
I found it worthwhile to look into the arguments for legalisation more closely, with the hope of sowing a little doubt in the minds of those who exhibit absolute certainty in the matter. This essay focuses on one point: the concept of “autonomy.”
(While there are several definitions of voluntary, involuntary, and non-voluntary euthanasia as well as assisted dying, assisted suicide, and physician assisted suicide, for the purposes of brevity in this essay, I use “assisted dying” throughout.)
Currently, in richer countries, arguments for legalising assisted dying frequently refer to the right to self-determination—or autonomy and free will. Our ability to self-determine seems to be unlimited and our right to it inviolable. The public’s response to opinion poll questions on voluntary euthanasia show that people can scarcely imagine not being able to make up their own minds, nor can they imagine not having the choice. Moreover, a healthy person answering a poll may have difficulty imagining being in a predicament where they simply would not wish to be given the choice.
I question whether self-determination is genuinely possible when choosing your own death. In my book, I explain that the choice will always be made in the context of a non-autonomous assessment of your quality of life—that is, an assessment outside your control. 1
All essential decisions that we make are made in relation to other people. Our decisions are affected by other people, and they affect other people. Although healthy people find it difficult to imagine themselves in situations where they do not decide freely, it is also true that all of us are vulnerable and dependent on others.
Yet autonomy in relation to assisted dying is often viewed in the same way as our fundamental right to choose our own course in life. If we are able to control our lives, then surely we can also control our death. Autonomy with respect to your own death, however, is already halved: you can choose to die if you don’t want to live, but you cannot choose to live if you are about to die.
Decisions about your own death are not made in normal day-to-day contexts. The wish to die arises against a backdrop: of desperation, a feeling of hopelessness, possibly a feeling of being superfluous. Otherwise, the wish would not be there. Thus, it is under these circumstances that the right to self-determination is exercised and the decision is made. Such a situation is a fragile basis for autonomy and an even more fragile basis for decision making. The choice regarding your own death is therefore completely different from most other choices usually associated with the concept of autonomy.
Here are just some of the critical matters that would arise if assisted dying were legalised.
A duty to die
The possibility of choosing to die would inhabit everyone’s consciousness—the patient, the doctor, the relatives, and the care staff—even if not formulated as an out-and-out offer. But if a law on assisted dying gives the patient a right to die, that right may turn into a duty to die. How autonomously can the weakest people act when the world around them deems their ill, dependent, and pained quality of life as beyond recovery?
Patients can find themselves directly or indirectly under duress to choose that option if they consider themselves sufficiently pained and their quality of life sufficiently low. Patients must be at liberty to choose assisted dying freely, of course—that is how it is presented—but the point is that the patient cannot get out of having to choose. It has been called the “prison of freedom.”
Internalised external pressure
Pressure on the patient does not have to be direct or articulated. As pointed out by the US professor of biomedical ethics Daniel Sulmasy it may exist as an “internalised external pressure.” 2 Likewise, the French bioethicist Emmanuel Hirsch states that individual autonomy can be an illusion. The theologian Nigel Biggar quotes Hirsch saying that a patient “may truly want to die, but this desire is not the fruit of his freedom alone, it may be—and most often is—the translation of the attitude of those around him, if not of society as a whole which no longer believes in the value of his life and signals this to him in all sorts of ways. Here we have a supreme paradox: someone is cast out of the land of the living and then thinks that he, personally, wants to die.” 3
The end of autonomy
An inherent problem of autonomy in connection with assisted dying is that a person who uses his or her presumed right to self-determination to choose death definitively precludes himself or herself from deciding or choosing anything. Where death is concerned, your right to self- determination can be exerted only by disposing of it for good. By your autonomy, in other words, you opt to no longer have autonomy. And those around must respect the right to self-determination. The respect refers to a person who is respected, but this is precisely the person who disappears.
Danish philosopher Johannes Sløk, who supported legalisation, said, “The actual concept of death has no content, for death is the same as nothing, and one cannot choose between life and nothing. Rather, therefore, one must speak of opting out; one opts out of life, without thereby choosing anything else. Death is not ‘something other’ than life; it is the cessation or annihilation of life.”
Autonomy is a consistent principle running through the care and management of patients and is enshrined in law. However, a patient’s autonomy means that he or she has the right to decline any treatment. It does not entail a right to have any treatment the patient might wish for. Patients do not have the right to demand treatment that signifies another’s duty to fulfil that right. If that were so, autonomy would be the same as “autocracy”—rule of the self over others. Even though patients have the right to reject any intervention, they do not have the right to demand any intervention. Rejecting any claim that the person might make is not a violation of a patient’s self- determination—for example, there may be sound medical reasons for not complying with a demand. The doctor also has autonomy, allowing him or her to say no. Refusing to kill a person or assist in killing cannot be a violation of that person’s autonomy.
The killing ban
Assisted dying requires the doctor’s moral and physical help. It is a binding agreement between two people: the one who is to be killed and the one who is to kill or assist in killing. But our society does not condone killing as a relationship between two legally competent, consenting people. Exemptions from the killing ban involve war or self-defence and are not justified on the grounds that the killing is done for the “benefit” of someone else.
Valuation of a life
If the action is to be decriminalised, as some people wish, it means the doctor will have to enter into deliberations and arguments for and against a request for assisted dying each time. That is, whether he or she is willing to grant it. The alternative would be to refer the patient to another doctor who might be willing to help—that doctor would still have to assess whether the patient’s life was worth preserving.
Thus, autonomy is not the only factor or even always the key factor when deciding whether assisted dying can be granted. It is not only the patient’s own evaluation that is crucial. The value of the patient’s life must also be assessed as sufficiently low. This demonstrates the limitation of the patient’s self-determination.
Relieving suffering
If a competent and legally capable person must have the option of voluntarily choosing assisted dying in the event of unbearable suffering, why does suffering have to be a requirement? The answer is straightforward: our concepts of assisted dying imply that compassion must form a crucial aspect of the decision—mercy killing and compassionate killing are synonyms. But this leads instantly to the question of why we should not also perform assisted dying on people who are not in a position to ask for it themselves but are also suffering.
Some people find the reasoning unproblematic. It stands to reason that relieving suffering is a duty after all. But in this context it is not unproblematic, because it effectively shifts the focus from the autonomy claimed. According to prevailing ideas about autonomy, patients initially evaluate their quality of life themselves, but ultimately it is those around them who end up gauging that quality and the value of their life. That is to say, the justification for assisted dying is borne on the premise that certain lives are not worth living rather than the presence of a request. The whole point is that in the process, respect for the right to self-determination becomes relative.
Autonomy is largely an illusion in the case of assisted dying. 1 A patient overwhelmed by suffering may be more in need of compassion, care, and love than of a kind offer to help end his or her life. It is not a question of whether people have a right to say that they are unworthy. It is a question of whether they have a right to be believed when saying it.
Ole Hartling is a physician of over 30 years standing, doctor of medical sciences at the University of Copenhagen, professor of health promotion at the University of Roskilde, and an author and co-author of several books and scientific articles published mainly in Scandinavia. Between 2000 and 2007 he was a member of the Danish Council of Ethics and its chair for five years. During this time, the council extensively debated the ethics of euthanasia and assisted dying.
Competing interests: I have read and understood BMJ policy on declaration of interests and have no relevant interests to declare.
- Gastmans C ,
- MacKellar C

- Table of Contents
- Random Entry
- Chronological
- Editorial Information
- About the SEP
- Editorial Board
- How to Cite the SEP
- Special Characters
- Advanced Tools
- Support the SEP
- PDFs for SEP Friends
- Make a Donation
- SEPIA for Libraries
- Entry Contents
Bibliography
Academic tools.
- Friends PDF Preview
- Author and Citation Info
- Back to Top
Voluntary Euthanasia
The entry sets out five conditions often said to be necessary for anyone to be a candidate for legalized voluntary euthanasia (and, with appropriate qualifications, physician-assisted suicide), outlines the moral case advanced by those in favor of legalizing voluntary euthanasia, and discusses the five most important objections made by those who deny that voluntary euthanasia is morally permissible and who are, in consequence, opposed to its being legalized.
1. Introduction
2. five conditions often proposed as necessary for candidacy for voluntary euthanasia, 3. a moral case for voluntary euthanasia, 4. five objections to the moral permissibility of voluntary euthanasia, other internet resources, related entries.
When a person performs an act of euthanasia, she brings about the death of another person because she believes the latter’s present existence is so bad that he would be better off dead, or believes that unless she intervenes and ends his life, his life will very soon become so bad that he would be better off dead. Accordingly, the motive of the person who performs an act of euthanasia is to benefit the one whose death is brought about. (This also holds for many instances of physician-assisted suicide, but use of the latter term is usually restricted to forms of assistance which stop short of the physician ‘bringing about the death’ of the patient, for example, those involving means that have to be activated by the patient.)
It is important to emphasize the motive of benefiting the person who is assisted to die because well-being is a key value in relation to the morality of euthanasia (see Section 3 below). Nonetheless, the defensibility of the contention that someone can be better off dead has been the subject of extensive philosophical deliberation. Those who claim that a person can be better off dead believe this to be true when the life that remains in prospect for that person has no positive value for her (a possibility which is discussed by e.g., Foot, 1977; McMahan 2002; Bradley 2009), whereas some of those who hold that a person’s life is inviolable deny that a person can ever be better off dead (e.g., Keown in Jackson and Keown 2012). A Kant-inspired variant on this latter position has been advanced by Velleman (1999). He considers that a person’s well-being can only matter if she is of intrinsic value and so that it is impermissible to violate a person’s rational nature (the source of her intrinsic value) for the sake of her well-being. Accordingly, he holds that it is impermissible to assist someone to die who judges that she would be better off dead and competently requests assistance with dying. The only exception is when a person’s life is so degraded as to call into question her rational nature, albeit he thinks it unlikely that anyone in that position will remain competent to request assistance with dying. This position appears to be at odds with the well-established right of a competent patient to refuse life-prolonging medical treatment, at least when further treatment is refused because she considers that her life no longer has value for her and further treatment will not restore its value to her. (For further reasons to reject arguments for the inviolability of the life of a person, including Velleman’s, see e.g., McMahan 2002; Young 2007; Sumner 2011, 2017.)
Because our concern will be with voluntary euthanasia – that is, with those instances of euthanasia in which a clearly competent person makes a voluntary and enduring request to be helped to die (or, by extension, when an authorised proxy makes a substituted judgment by choosing in the manner the no-longer-competent person would have chosen had he remained competent) – a second key value is the competence of the person requesting assistance with dying. There will be occasion to mention non-voluntary euthanasia – instances of euthanasia where a person lacks the competence at the time when a decision is to be made to request euthanasia and has not previously competently declared a preference for it via an advance directive (see the entry on advance directives ) – only when consideration is given to the claim that permitting voluntary euthanasia will lead via a slippery slope to permitting non-voluntary euthanasia. Nothing will be said here about involuntary euthanasia , where a competent person’s life is brought to an end despite an explicit expression of opposition to euthanasia, beyond saying that, no matter how honorable the perpetrator’s motive, such a death is, and ought to be, unlawful.
Debate about the morality and legality of voluntary euthanasia has been, for the most part, a phenomenon of the second half of the twentieth century and the beginning of the twenty first century. Certainly, the ancient Greeks and Romans did not believe that life needed to be preserved at any cost and were, in consequence, tolerant of suicide when no relief could be offered to a dying person or, in the case of the Stoics and Epicureans, when a person no longer cared for his life. In the sixteenth century, Thomas More, in describing a utopian community, envisaged such a community as one that would facilitate the death of those whose lives had become burdensome as a result of ‘torturing and lingering pain’. But it has only been in the last hundred years that there have been concerted efforts to make legal provision for voluntary euthanasia. Until quite recently there had been no success in obtaining such legal provision (though assisted suicide, including, but not limited to, physician-assisted suicide, has been legally tolerated in Switzerland for a number of decades). However, the outlook changed dramatically in the 1970s and 80s because of a series of court cases in the Netherlands which culminated in an agreement between the legal and medical authorities to ensure that no physician would be prosecuted for assisting a patient to die as long as certain guidelines were strictly adhered to (see Griffiths, et al., 1998). In brief, the guidelines were established to permit physicians to practise voluntary euthanasia in those instances in which a competent patient had made a voluntary and informed request to be helped to die, the patient’s suffering was unbearable, there was no way of making that suffering bearable that was acceptable to the patient, and the physician’s judgements as to diagnosis and prognosis were confirmed after consultation with another physician.
The first legislative approval for voluntary euthanasia was achieved with the passage in the parliament of Australia’s Northern Territory of a bill enabling physicians to practise voluntary euthanasia. Subsequent to the Act’s proclamation in 1996, it faced a series of legal challenges from opponents of voluntary euthanasia. In 1997 the challenges culminated in the Australian National Parliament overturning the legislation when it prohibited Australian territories from enacting legislation to permit voluntary euthanasia on constitutional grounds. Australia is a federation consisting of six states and two territories. Unlike the territories, the states do have the constitutional right to enact such legislation and in 2017 the state of Victoria did just that. The legislation came into effect in 2019. In 2019, a second state, Western Australia, enacted legislation to enable voluntary medically assisted death. The legislation became effective in 2021. In 2021 three further states, Tasmania, South Australia and Queensland enacted legislation to enable voluntary medically assisted death which came into force in 2022 for the first two, and 2023 for the third. Finally, in 2022 NSW enacted legislation which came into force in 2023 resulting in voluntary medically assisted death being available in each of the states. Attempts are currently being made in both the Australian Capital Territory and the Northern Territory to introduce legislation in favor of voluntary medically assisted death that will avoid being vetoed by the federal parliament.
In November 2000, the Netherlands passed legislation to legalize the practice of voluntary euthanasia. The legislation passed through all the parliamentary stages early in 2001. The Belgian parliament passed similar legislation in 2002 and Luxembourg followed suit in 2009. (For a very helpful comparative study of relevant legislation see Lewis 2007. See also Griffiths, et al. 2008.)
In Oregon in the United States, legislation was introduced in 1997 to permit physician-assisted suicide after a referendum strongly endorsed the proposed legislation. Later in 1997 the Supreme Court of the United States ruled that there is no constitutional right to physician-assisted suicide; however, the Court did not preclude individual states from legislating in favor of physician-assisted suicide (so the Oregon legislation was unaffected). Since that time the Oregon legislation has been successfully utilised by a significant number of people and similar legislation has been passed in the state of Washington in 2009, in Vermont in 2013, and more recently still in California, Colorado, Florida, Hawaii, Iowa, Maine, Maryland, Massachusetts, Minnesota, New Jersey, New Mexico and the District of Columbia. A series of judicial decisions in the state of Montana in 2008 and 2009 established that the state could not prohibit physician-assisted suicide but legislation has not yet been introduced to codify the legal situation. A number of the remaining states are currently considering physician-assisted suicide bills.
A similar legal position to that in Montana obtained in the nation of Colombia from the late 1990s as a result of a majority ruling by its Constitutional Court in favor of the legality of physician-assisted suicide but legislative provision was finally made only quite recently. In 2021, Spain legalized voluntary euthanasia. In Austria and Germany courts have authorised physician-assisted suicide but no legislative backing for the practice has been introduced, while in Italy legislation for voluntary medically assisted death has been passed in one house of the bicameral parliament. In Portugal legislation for physician-assisted suicide was passed but was subsequently rejected by the Constitutional Court.
In Canada, the province of Quebec introduced legislation permitting medical aid in dying in 2014. The legislation came into effect in 2016 at around the same time that the Canadian National Parliament passed legislation permitting both physician-assisted suicide and voluntary euthanasia throughout all of the Canadian federation. (For a brief account of events leading up to the enactment of the various pieces of legislation in Canada see Downie and Schuklenk 2021.)
New Zealand held a referendum in 2019 which resulted in approval for the introduction of legislation for voluntary medically assisted death. The legislation came into effect late in 2021.
In the following countries legislative proposals for voluntary medically assisted death are presently under review: the Czech Republic, France, Ireland, the Isle of Man, Japan, Jersey, South Korea, the Philippines, Slovenia and the United Kingdom.
With that brief sketch of the historical background in place, we will proceed first to consider the conditions that those who have advocated making voluntary medically assisted death legally permissible have typically insisted should be satisfied. Consideration of the proposed conditions will establish a framework for the moral interrogation that will follow in Sections 3 and 4. Section 3 will outline the positive moral case put forward by those who want voluntary euthanasia and physician-assisted suicide to be legally permissible. Section 4 will be devoted to scrutinising the most important of the objections that have been levelled against that case by those opposed to the legalization of voluntary euthanasia and physician-assisted suicide.
Advocates of voluntary euthanasia typically contend that if a person
- is suffering from a terminal illness;
- is unlikely to benefit from the discovery of a cure for that illness during what remains of her life expectancy;
- is, as a direct result of the illness, either suffering intolerable pain, or only has available a life that is unacceptably burdensome (e.g., because the illness has to be treated in ways that lead to her being unacceptably dependent on others or on technological means of life support);
- has an enduring, voluntary and competent wish to die (or has, prior to losing the competence to do so, expressed a wish to be assisted to die in the event that conditions (a)-(c) are satisfied); and
- is unable without assistance to end her life,
there should be legal and medical provision to facilitate her being allowed to die or assisted to die.
It should be acknowledged that these conditions are quite restrictive, indeed more restrictive than many think appropriate. In particular, the first condition restricts access to voluntary euthanasia to those who are terminally ill . While that expression is not free of all ambiguity, for present purposes it can be agreed that it does not include those who are rendered quadriplegic as a result of accidents, or sufferers from chronic diseases, or individuals who succumb to forms of dementia like Alzheimer’s Disease, to say nothing of those afflicted by ‘existential suffering’. Those who consider that cases like these show the first condition to be too restrictive (e.g., Varelius 2014, Braun, 2023) may, nonetheless, agree that including them as candidates for legalized voluntary euthanasia is likely to make it far harder in many jurisdictions to gain sufficient support for legalization (and so to make it harder to help those terminally ill persons who wish to die). Even so, they believe that voluntary euthanasia should be permitted for those who consider their lives no longer worth living, not just for for the terminally ill. Whether those who judge that their lives are no longer worth living, and so believe their lives are in that sense ‘complete’, should be afforded medical assistance with dying, has recently become a pressing concern in Belgium and the Netherlands. Several court cases have affirmed that such assistance may sometimes be provided for individuals in the former category even though the question remains as to whether it is properly a medical responsibility to render assistance with dying to someone who believes her life is complete despite her not suffering from a terminal medical condition (see, e.g., Young 2017). Relatedly, the issues of whether those suffering from a disability which will not reasonably foreseeably lead to death and those suffering because of a mental illness should be able to access medical assistance with dying have recently been the subject of intense debate in Canada. The debate culminated in disabled individuals, whose conditions are the cause of enduring, intolerable and irremediable suffering, being given access to medical assistance with dying as long as they are capable of making a competent request for that assistance. An intention to make a similar arrangement for those whose sole underlying condition is a mental illness was flagged for introduction in 2024, but has been temporarily shelved until further research has been conducted on the issue. It seems likely that the changes that have been made, or mooted, in these jurisdictions to the eligibility conditions for medical assistance with dying will lead to an expansion of the eligibility conditions for voluntary medically assisted death in other jurisdictions.
The fifth condition further restricts access to voluntary euthanasia by excluding those capable of ending their own lives, and so may be thought unduly restrictive by those who would wish to discourage terminally ill patients from attempting suicide. There will be yet others who consider this condition to be too restrictive because competent patients can always refuse nutrition and hydration (see, e.g., Bernat, et al. 1993; Savulescu 2014). Though this is true, many competent dying persons still wish to have access to legalized medically assisted death, rather than having to rely on refusing nutrition and hydration, so that they may retain control over the timing of their deaths and avoid needlessly prolonging the process of dying.
The second condition is intended simply to reflect the fact that it is normally possible to say when someone’s health status is incurable. So-called ‘miracle’ cures may be proclaimed by sensationalist journalists, but progress toward medical breakthroughs is typically painstaking. If there are miracles wrought by God that will be quite another matter entirely, but it is at least clear that not everyone’s death is thus to be staved off.
The third condition recognises what many who oppose the legalization of voluntary euthanasia do not, namely, that it is not only a desire to be released from pain that leads people to request help with dying. In the Netherlands, for example, pain has been found to be a less significant reason for requesting assistance with dying than other forms of suffering like frustration over loss of independence (see e.g., Marquet, et al. 2003; Onwuteaka-Philipsen, et al. 2012; Emanuel, et al. 2016). Sufferers from some terminal conditions may have their pain relieved but have to endure side effects that, for them, make life unbearable. Others may not have to cope with pain but, instead, with having to rely on forms of life support that simultaneously rob their lives of quality (as with, e.g., motor neurone disease). Yet others struggle with psychological distress and various psychiatric conditions and believe these conditions ought to be counted among the forms of suffering that qualify competent individuals to access medical assistance with dying. There has been greater recognition of, and support for, this position in those jurisdictions that make the role of unbearable suffering central to the determination of the eligibility of competent individuals for medical assistance with dying (see the discussion above of the first condition). Even so, inclusion of these forms of suffering highlights legitimate issues to do with the competence of at least some of those who suffer from them. (For a helpful recent study of the handling of requests for assistance with dying by psychiatric patients in the Netherlands see Kim, et al. 2016.)
A final preliminary point is that the fourth condition requires that the choice to die not only be uncoerced and competent but that it be enduring. The choice is one that will require time for reflection, and, almost certainly, discussion with others, so should not be settled in a moment. Nonetheless, as with other decisions affecting matters of importance, adults are presumed to choose voluntarily and to be competent unless the presence of defeating considerations can be established. (See the entry on decision-making capacity .) The burden of proof of establishing lack of voluntariness, or lack of competence, is on those who refuse to accept an adult person’s choice. There is no need to deny that this burden can sometimes be met (e.g., by pointing to the person’s being in a state of clinical depression). The claim is only that the onus falls on those who assert that an adult’s choice is not competent. (There are different issues to be faced when the competence of at least some older children and adolescents is at issue. In the Netherlands, for example, those aged twelve and older have sometimes been found to be competent to make end-of-life decisions for themselves. However, the topic will not be pursued further here because the focus of the entry is on competent adults.)
Clearly the five conditions set out above are likely to require some refinement if complete agreement is to be reached but there is sufficient agreement for us to proceed without further ado to consideration of the cases for and against legalization of voluntary euthanasia. (However, for a fuller discussion of issues concerning the definition of ‘euthanasia’ see, e.g., Beauchamp and Davidson 1979.)
One central ethical contention in support of voluntary euthanasia is that respect for persons demands respect for their autonomous choices as long as those choices do not result in harm to others. Respect for people’s autonomous choices is directly connected with the requirement for competence because autonomy presupposes competence (cf., Brock 1992). People have an interest in making important decisions about their lives in accordance with their own conception of how they want to live. In exercising autonomy, or self-determination, individuals take responsibility for their lives; since dying is a part of life, choices about the manner of their dying and the timing of their death are, for many people, part of what is involved in taking responsibility for their lives. Many are concerned about what the last phase of their lives will be like, not merely because of fears that their dying might involve them in great suffering, but also because of the desire to retain their dignity, and as much control over their lives as possible, during this phase. A second contention in support of voluntary euthanasia was mentioned at the beginning of this entry, namely the importance of promoting the well-being of persons. When someone is suffering intolerable pain or only has available a life that is unacceptably burdensome (see the third condition above), and he competently requests medical assistance with dying, his well-being may best be promoted by affording him that assistance. When harnessed together, the value to individuals of making autonomous choices, and the value to those individuals who make such choices of promoting their own well-being, provide the moral foundation for requests for voluntary euthanasia. Each consideration is necessary for moral justification of the practice, but taken in isolation neither suffices (see, e.g., Young 2007, 2017; Sumner 2011, 2017).
The technological interventions of modern medicine have had the effect of stretching out the time it takes for many people to die. Sometimes the added life this brings is an occasion for rejoicing; sometimes it drags out the period of significant physical and intellectual decline that a person undergoes with the result that life becomes no longer worth living. Many believe there is no single, objectively correct answer as to when, if at all, a person’s life becomes a burden and hence unwanted. If they are right, that simply points up the importance of individuals being able to decide autonomously for themselves whether their own lives retain sufficient quality and dignity to make life worth living. Others maintain that individuals can be in error about whether their lives continue to be worth living (cf., Foot 1977). The conditions outlined above in Section 2 are intended by those who propose them to serve, among other purposes, to safeguard against such error. But it is worth adding that in the event that a person who considers that she satisfies those conditions is judged by her medical attendants to be in error about whether it would be worth her continuing to live, the likely outcome is that those attendants will refuse to provide medical assistance with dying. (Evidence that will be mentioned below shows that this happens more frequently than might be predicted in jurisdictions in which medically assisted dying has been legalized. (There are discussions of the principles at stake in such matters in Young 2007; Wicclair 2011; Sumner 2020.) Unless a patient is able to be transferred to the care of other medical professionals who accept her assessment, she will have to rely on her own resources (e.g., by refusing nutrition and hydration). Even so, other things being equal, as long as a critically ill person is competent, her own judgement of whether continued life is a benefit to her ought to carry the greatest weight in any end-of-life decision making regardless of whether she is in a severely compromised and debilitated state. The idea that a competent individual’s autonomous judgment of the value to her of continued life should trump an assessment by others of her well-being should not be thought surprising because precisely the same happens when a competent patient refuses life-prolonging treatment.
Suppose, for the sake of argument, that it is agreed that we should respect a person’s competent request for medical assistance with dying (e.g., so as to enable her to achieve her autonomously chosen goal of an easeful death). It might be thought that in such an eventuality different moral concerns will be introduced from those that arise in connection with competent refusals. After all, while competent patients are entitled to refuse any form of medical treatment, they are not entitled to insist on the administration of forms of medical treatment that have no prospect of conferring a medical benefit or are not being provided because of a scarcity of medical resources or their affordability. While each of these points is sound, it remains the case that medical personnel have a duty to relieve suffering when that is within their capacity. Accordingly, doctors who regard medical assistance with dying as an element of appropriate medical care will consider it morally permissible to agree to a request for assistance with dying by a competent dying patient who wishes to avoid unbearable suffering. The reason for claiming only that this is morally permissible rather than morally obligatory will be explained in a subsequent paragraph. (For further reflections on the issue of responses to requests for medical assistance see, for instance, Dworkin 1998; Sumner 2011, 2017, 2020; Young 2007, 2017.)
Notwithstanding this response, as was seen earlier, at least some proponents of voluntary medically assisted dying wish to question why medical assistance with dying should be restricted to those covered by, in particular, the first three conditions set out above in Section 2. If people’s competent requests for medically assisted death should be respected why impose any restrictions at all on who may have access to medically assisted death? Why, for example, should those suffering from depression, or forms of dementia, not be eligible for medically assisted dying? Most proponents of voluntary medically assisted dying hold that there are at least two reasons for restricting access to it to those who satisfy the conditions set out earlier (or, a modified set that takes account of the concerns canvassed in the discussion of those proposed conditions). First, they contend that there are political grounds for doing so, namely, that because legalizing medically assisted dying for competent individuals is politically contested, the best hope for its legalization lies in focusing on those forms of suffering most likely to effect law reform. That is why some proponents deny the eligibility even of sufferers from conditions like ‘locked-in’ syndrome, motor neurone disease, and multiple sclerosis for voluntary medically assisted dying since, strictly, they are not terminally ill, and reliance has to be placed in consequence on their claim to be suffering unbearably. Second, and relatedly, most proponents of the legalization of medical assistance with dying have been cautious about supporting medically assisted death for those suffering from, for example, depression and dementia, because not only are they not terminally ill, but their competence to request assistance with dying is apt to be called into question, particularly in instances where they have given no prior indication of their preference for such assistance. Restricting access to medical assistance with dying to those whose suffering is less likely to be disputed avoids becoming embroiled in controversy. As was noted earlier, some critics of the restrictive approach (e.g., Varelius 2014) take a harder line and claim that it should not even be necessary for a person to be suffering from a medical condition to be eligible for medical assistance with dying; it should be enough to be ‘tired of life’. Only in a few jurisdictions, viz., Switzerland, the Netherlands and Belgium, has this issue been seriously broached. Regardless of what may happen in those jurisdictions, those seeking the legal provision of medical assistance with dying in other jurisdictions seem likely to maintain that if such assistance is to be seen as a legitimate form of medical care it has to be provided in response to a medical condition (rather than because someone is ‘tired of life’), and, indeed, restricted to those who satisfy the conditions outlined earlier in Section 2 (or some similar set of conditions). In short, these latter hold that making an autonomous request for assistance with dying is necessary, but should not be sufficient, for triggering such assistance.
There is one final matter of relevance to the moral case for voluntary medically assisted death on which comment must be made. The comment concerns a point foreshadowed in a previous paragraph, but it is also linked with the remark just made about the insufficiency of an autonomous request for assistance with dying to trigger that assistance. It is important to make the point that respect has to be shown not only for the dying person’s autonomy but also for the professional autonomy of any medical personnel asked to lend assistance with dying. The value (or, as some would prefer, the right) of self-determination does not entitle a patient to try to compel medical professionals to act contrary to their own moral or professional values. Hence, if voluntary euthanasia is to be legally permitted, it must be against a backdrop of respect for professional autonomy. Similarly, if a doctor’s view of her moral or professional responsibilities is at odds with her patient’s competent request for euthanasia, she should make provision, where it is feasible to do so, for the transfer of the patient to the care of a doctor who faces no such conflict. Given that, to date, those who contend that no scope should be permitted for conscientious objection within medical practice have garnered very little support for that view, making use of referrals and transfers remains the most effective means of resolving such disagreements.
Opponents of voluntary euthanasia have endeavored in a variety of ways to counter the very straightforward moral case that has been laid out above for its legalization (see, for example, Keown 2002; Foley, et al. 2002; Biggar 2004; Gorsuch 2006). Some of the counter-arguments are concerned only with whether the moral case warrants making the practice of voluntary euthanasia legal, whereas others are concerned with trying to undermine the moral case itself. In what follows, consideration will be given to the five most important counter-arguments. (For more comprehensive discussions of the morality and legality of medically assisted death see Biggar 2004; Gorsuch 2006; Young 2007; Sumner 2011, 2017; Keown 2018).
4.1 Objection 1
It is sometimes said (e.g., Emanuel 1999; Keown in Jackson and Keown 2012) that it is not necessary nowadays for people to die while suffering from intolerable or overwhelming pain because the provision of effective palliative care has improved steadily, and hospice care is more widely available. Some have urged, in consequence, that voluntary euthanasia is unnecessary.
There are several flaws in this contention. First, while both good palliative care and hospice care make important contributions to the care of the dying, neither is a panacea. To get the best palliative care for an individual involves trial and error, with some consequent suffering in the process; moreover, even the best care fails to relieve all pain and suffering. Perhaps even more importantly, high quality palliative care commonly exacts a price in the form of side-effects such as nausea, incontinence, loss of awareness because of semi-permanent drowsiness, and so on. A rosy picture is often painted as to how palliative care can transform the plight of the dying. Such a picture is misleading according to those who have closely observed the effect of extended courses of treatment with drugs like morphine. For these reasons many skilled palliative care specialists acknowledge that palliative care does not enable an easeful death for every patient. Second, even though the sort of care provided through hospices is to be applauded, it is care that is available to only a small proportion of the terminally ill and then usually only in the very last stages of the illness (typically a matter of a few weeks). Notwithstanding that only relatively few of the dying have access to hospice care it is worth drawing attention to the fact that in, Oregon, to cite one example, a high proportion of those who have sought physician-assisted suicide were in hospice care. Third, and of greatest significance for present purposes, not everyone wishes to avail themselves of palliative or hospice care. For those who prefer to die on their own terms and in their own time, neither option may be attractive. As previously mentioned, a major source of distress for many dying patients is the frustration that comes with being unable to satisfy their autonomous wishes. Fourth, as also indicated earlier, the suffering that occasions a desire to end life is not always traceable to pain caused by illness. For some, what is intolerable is their forced dependence on others or on life-supporting machinery; for these patients, the availability of effective pain control is not the primary concern. (In relation to the preceding matters see Rietjens, et al. 2009 and Onwuteaka-Philipsen et al. 2012 for findings for the Netherlands; and, for Oregon, Ganzini, et al. 2009.)
4.2 Objection 2
A second, related objection to the moral and legal permissibility of voluntary euthanasia turns on the claim that we can never have sufficient evidence to be justified in believing that a dying person’s request to be helped to die is competent, enduring and genuinely voluntary.
It is certainly true that a request to die may not reflect an enduring desire to die (just as some attempts to commit suicide may reflect only temporary despair). That is why advocates of the legalization of voluntary euthanasia have argued that a cooling off period should normally be required before euthanasia is permitted to ensure that the request is enduring. That having been said, to claim that we can never be justified in believing that someone’s request to die reflects a settled preference for death is to go too far. If a competent person discusses the issue with others on different occasions over time, and remains steady in her resolve, or privately reflects on the issue for an extended period and does not waver in her conviction, her wish to die surely must be counted as enduring.
But, it might be asked, what if a person is racked with pain, or mentally confused because of the measures taken to relieve her pain, and is, in consequence, unable to think clearly and rationally about the alternatives? It has to be agreed that a person in those circumstances who wants to die should not be assumed to have a truly voluntary and enduring desire to die. However, there are at least two important points to make about those in such circumstances. First, they do not account for all of the terminally ill, so even if it is acknowledged that such people are incapable of agreeing to voluntary euthanasia that does not show that no one can ever voluntarily request help to die. Second, it is possible in at least some jurisdictions for a person to indicate, in advance of losing the capacity to give competent consent, how she would wish to be treated should she become terminally ill and suffer either intolerable pain or an unacceptable loss of control over her life (cf., for instance, Dworkin 1993). ‘Living wills’ or ‘advance directives’ are legal instruments for giving voice to people’s wishes while they are capable of giving competent, enduring and voluntary consent, including to their wanting help to die. As long as they are easily revocable in the event of a change of mind (just as civil wills are), they should be respected as evidence of a well thought-out conviction. (For more detailed consideration of these instruments see the entry on advance directives .)
Perhaps, though, what is really at issue in this objection is whether anyone can ever form a competent, enduring and voluntary judgement about being better off dead, rather than continuing to suffer from an illness, prior to suffering such an illness (cf., Keown in Jackson and Keown 2012). If this is what underlies the objection it is surely too paternalistic to be acceptable. Why is it not possible for a person to have sufficient inductive evidence (e.g., based on the experience of the deaths of friends or family) to know her own mind, and act accordingly, without having had direct experience of such suffering?
4.3 Objection 3
According to the traditional interpretation of the ‘doctrine of double effect’ it is permissible to act in a way which it is foreseen will have a bad effect, provided only that
- the bad effect occurs as a side-effect (i.e., indirectly) to the achievement of the act that is directly aimed at;
- the act directly aimed at is itself morally good or, at least, morally neutral;
- the good effect is not achieved by way of the bad, that is, the bad must not be a means to the good; and
- the bad effect must not be so serious as to outweigh the good effect.
Hence, it is permissible, according to the doctrine of double effect, to, for example, alleviate pain (a good effect) by administering a drug such as morphine, knowing that doing so will shorten life, but impermissible to administer the same drug with the direct intention of terminating a patient’s life (a bad effect). This latter claim is said to apply regardless of whether the drug is given at the person’s request.
This is not the appropriate forum for a full consideration of the doctrine, for which see the entry on the doctrine of double effect . However, there is one very important criticism to be made of the application of the doctrine that has direct relevance to the issue of voluntary euthanasia.
On the most plausible reading, the doctrine of double effect can be relevant to the permissibility of voluntary euthanasia only when a person’s death is bad for her or, to put it another way, a harm to her. Sometimes the notion of ‘harm’ is understood simply as damage to a person’s interests whether consented to or not. At other times, it is understood, more strictly, as damage that has been wrongfully inflicted. On either understanding of harm, there can be instances in which death for a person does not constitute a harm for her because it will either render her better off, or, as some would insist, no worse off, when compared with remaining alive. Accordingly, in those instances, the doctrine of double effect can have no relevance to the debate about the permissibility of voluntary euthanasia. (For extended discussions of the doctrine of double effect and its bearing on the moral permissibility of voluntary euthanasia see, e.g., McIntyre 2001; Woodward 2001; Cavanaugh 2006; Young 2007; Sumner 2011, 2017.)
4.4 Objection 4
As was noted earlier in Section 3, there is a widespread belief that so-called passive (voluntary) euthanasia, wherein life-sustaining or life-prolonging measures are withdrawn or withheld in response to a competent patient’s request, is morally permissible. The reason why passive (voluntary) euthanasia is said to be morally permissible is that the patient is simply allowed to die because steps are not taken to preserve or prolong life. This happens, for example, when a dying patient requests the withdrawal or the withholding of measures whose administration would be medically futile, or unacceptably burdensome. By contrast, active (voluntary) euthanasia is said to be morally impermissible because it is claimed to require an unjustifiable intentional act of killing to satisfy the patient’s request (cf., for example, Finnis, 1995; Keown in Jackson and Keown 2012; Keown 2018).
Despite its popularity and widespread use, the distinction between passive and active euthanasia is neither particularly clear nor morally helpful. (For a fuller discussion, see McMahan 2002.) Whether behavior is described in terms of acts or omissions (a distinction which underpins the alleged difference between active and passive voluntary euthanasia and that between killing a person and letting her die), is often a matter of pragmatics rather than anything of deeper moral importance. Consider, for instance, the practice (once common in hospitals) of deliberately proceeding slowly to a ward in response to a request to provide assistance for a patient who has been assigned a ‘not for resuscitation’ code. Or, consider ‘pulling the plug’ on a respirator keeping an otherwise dying patient alive, as against not replacing the oxygen supply when it runs out. Are these acts or omissions? If the answers turn on merely pragmatic considerations the supposed distinction between passive euthanasia and active euthanasia will be hard to sustain.
Even supposing that the distinction between acts and omissions, and the associated distinction between killing and letting die, can be satisfactorily clarified (on which see the entry doing v. allowing harm ), there remains the issue of whether these distinctions have moral significance in every circumstance. Consider a case of a patient suffering from motor neurone disease who is completely respirator dependent, finds her condition intolerable, and competently and persistently requests to be removed from the respirator so that she may die. Even the Catholic Church in recent times has been prepared to agree that it is permissible, in a case like this, to turn off the respirator. No doubt this has been because the Catholic Church considers such a patient is only being allowed to die. Even were it to be agreed, for the sake of argument, that such a death should be regarded as an instance of letting die, this concession would not show that it would have been morally worse had the patient been killed at her request (active voluntary euthanasia) rather than being allowed to die (passive voluntary euthanasia). Indeed, supporters of voluntary medically assisted death maintain that since death is beneficial in such an instance (or, at the very least, leaves the dying person no worse off), actively bringing about the death is morally to be preferred to just allowing it to happen because the desired benefit is achieved sooner and thus with less suffering.
Opponents of voluntary euthanasia claim, however, that the difference between active and passive euthanasia is to be found in the agent’s intention: if someone’s life is intentionally terminated she has been killed, whereas if she is just no longer being aggressively treated, her death should be attributed to the underlying disease. Many physicians would say that their intention in withholding or withdrawing life-sustaining medical treatment in such circumstances is simply to respect the patient’s wishes. This is plausible in those instances where the patient competently requests that aggressive treatment no longer be given (or, the patient’s proxy makes such a request). But it will often be implausible. In many cases the most plausible interpretation of a physician’s intention in withholding or withdrawing life-sustaining measures is that it is to end the patient’s life. Consider the palliative care practice of ‘terminally sedating’ a patient after a decision has been made to cease aggressive treatment. Suppose (as sometimes happens) that this is then followed by withholding artificially supplied nutrition. In these latter instances the best explanation of the physician’s behavior is that the physician intends thereby to end the life of the patient. What could be the point of the action, the goal aimed at, the intended outcome, if not to end the patient’s life? (Cf. Winkler 1995.) No sense can be made of the action as being intended to palliate the patient’s diseased condition, or to keep the patient comfortable. Nor is it appropriate to claim that what kills the patient is the underlying disease. What kills the patient is the act of depriving her of nutrition (i.e., of starving her to death). The point can be generalized to cover many more instances involving either the withdrawal or the withholding of life-sustaining medical treatment. In short, there is no good reason to think that whereas so-called passive voluntary euthanasia is morally acceptable active voluntary euthanasia never can be.
But we can go further. Giving titrated doses of morphine that reach levels beyond those needed to control pain, or removing a respirator from a sufferer from motor neurone disease, seem to many of us to amount to intentionally bringing about the death of the person being cared for. To be sure, as was acknowledged above, there are circumstances in which doctors can truthfully say that the actions they perform, or omissions they make, will bring about the deaths of their patients even though it was not their intention that those patients would die. So, for instance, if a patient refuses life-prolonging medical treatment because she considers it futile, it can be reasonable to say that her doctor’s intention in complying with the request was simply to respect her wishes. Nevertheless, as we have seen, there are other circumstances in which it is highly stilted to claim, as some doctors continue to do, that they had no intention of bringing about death.
These considerations should settle matters but do not do so for those who maintain that killing, in medical contexts, is always morally unjustified – a premise that underwrites much of the debate surrounding this fourth objection. But this underlying assumption is open to challenge and has been challenged by, for instance, Rachels 1986 and McMahan 2002. One of the reasons the challengers have given is that there are cases in which killing a competent dying person when she requests assistance with dying, is morally preferable to allowing her to die, namely, when taking the latter option would serve only to prolong her suffering against her wishes. Further, despite the longstanding legal doctrine that no one can justifiably consent to be killed (on which more later), it surely is relevant to the justification of an act of killing that the person killed has autonomously decided that she would be better off dead and so asks to be helped to die.
4.5 Objection 5
It is sometimes said that if society allows voluntary euthanasia to be legalized, we will then have set foot on a slippery slope that will lead us eventually to support other forms of euthanasia, including, in particular, non-voluntary euthanasia. Whereas it was once the common refrain that that was precisely what happened in Hitler’s Germany, in recent decades the tendency has been to claim that experience with legalized euthanasia in the Netherlands and Belgium, in particular, has confirmed the reality of the slippery slope.
Slippery slope arguments come in various versions. One (but not the only) way of classifying them has been to refer to logical, psychological and arbitrary line versions. The common feature of the different forms is the contention that once the first step is taken on a slippery slope the subsequent steps follow inexorably, whether for logical reasons, psychological reasons, or to avoid arbitrariness in ‘drawing a line’ between a person’s actions. (For further discussion see, e.g., Rachels 1986; Brock 1992; Walton 1992.)
We need first to consider whether, at the theoretical level, any of these forms of argument is powerful enough to refute the case for the legalization of voluntary euthanasia. We will then be in a position to comment on the alleged empirical support from the experiences of Hitler’s Germany and, more recently, of legalized euthanasia in the Netherlands and elsewhere, for the existence of a slippery slope that supposedly comes into being with the legalization of voluntary euthanasia.
To begin with, there is nothing logically inconsistent in supporting voluntary euthanasia while maintaining the moral inappropriateness of non-voluntary euthanasia. (However, for an attempt to press the charge that there is such an inconsistency see, e.g., Keown 2022.) Undoubtedly, some advocates of voluntary euthanasia wish also to lend their support to some acts of non-voluntary euthanasia, for example, for those in persistent vegetative states who have never indicated their wishes about being helped to die, or for certain severely disabled infants for whom the outlook is hopeless. (See, e.g., Kuhse and Singer 1985; Singer 1994; Stingl 2010; Sumner 2017.) Others believe that the consent of the patient is strictly required if euthanasia is appropriately to be legalized. The difference is not a matter of logical acumen; it is to be explained by reference to the importance placed on key values by the respective supporters. Thus, for example, those who insist on the necessity for a competent request by a patient for medical assistance with dying typically believe that such a request is the paramount consideration in end-of-life decision making (even when it is harnessed to the value of individual well-being), whereas those who consider a person’s best interests to be the paramount consideration are more likely to believe in the justifiability of instances of non-voluntary euthanasia like those mentioned above.
Next, it is hard to see why moving from voluntary to non-voluntary euthanasia is supposed to be psychologically inevitable. Why should those who support the legalization of voluntary euthanasia, because they value the autonomy of the individual, find it psychologically easier, in consequence, to endorse the killing of those who are not able competently to request assistance with dying? What reason is there to believe that they will, as a result of their support for voluntary euthanasia, be psychologically driven to endorse a practice of non-voluntary euthanasia?
Finally, since there is nothing arbitrary about distinguishing voluntary euthanasia from non-voluntary euthanasia (because the line between them is based on clear principles), there can be no substance to the charge that only by arbitrarily drawing a line between them could non-voluntary euthanasia be avoided were voluntary euthanasia to be legalized.
What, though, of Hitler’s Germany and the recent experience of legalized voluntary euthanasia in the Netherlands and elsewhere? The former is easily dismissed as an indication of an inevitable descent from voluntary euthanasia to non-voluntary. There never was a policy in favor of, or a legal practice of, voluntary euthanasia in Germany in the 1920s to the 1940s (see, for example, Burleigh 1994). There was, prior to Hitler coming to power, a clear practice of killing some disabled persons. But it was never suggested that their being killed was justified by reference to their best interests; rather, it was said that society would be benefited. Hitler’s later revival of the practice and its widening to take in other groups such as Jews and gypsies was part of a program of eugenics , not euthanasia.
Since the publication of the Remmelink Report in 1991 into the medical practice of euthanasia in the Netherlands, it has frequently been said that the Dutch experience shows that legally protecting voluntary euthanasia is impossible without also affording shelter to the non-voluntary euthanasia that will follow in its train (see, e.g., Keown 2018). In the period since that report there have been regular national studies of the practice of euthanasia in the Netherlands (see, e.g., Rietjens, et al. 2009; Onwuteaka-Philipsen, et al. 2012; van der Heide, et al. 2017). The findings from these national studies have consistently shown that there is no evidence for the existence of such a slippery slope. Among the specific findings the following are worth mentioning: of those terminally ill persons who have been assisted to die about sixty per cent have clearly been cases of voluntary euthanasia as it has been characterised in this entry; of the remainder, the vast majority of cases were of patients who at the time of their medically assisted deaths were no longer competent. It might be thought that these deaths ought to be regarded as instances of non-voluntary euthanasia. But, in fact, it would be inappropriate to regard them as such. Here is why. For the overwhelming majority of these cases, the decisions to end life were taken only after consultation between the attending doctor(s) and close family members, and so can legitimately be thought of as involving substituted judgements. Moreover, according to the researchers, the overwhelming majority of these cases fit within either of two common practices that occur in countries where voluntary euthanasia has not been legalized, namely, that of terminal sedation of dying patients, and that of giving large doses of opioids to relieve pain while foreseeing that this will also end life. In a very few cases, there was no consultation with relatives, though in those cases there were consultations with other medical personnel. The researchers contend that these instances are best explained by the fact that families in the Netherlands strictly have no final legal authority to act as surrogate decision-makers for incompetent persons. For these reasons the researchers maintain that non-voluntary euthanasia is not widely practised in the Netherlands.
That there have only been a handful of prosecutions of Dutch doctors for failing to follow agreed procedures (Griffiths, et al. 1998; Asscher and van de Vathorst 2020), that none of the doctors prosecuted has had a significant penalty imposed, that a significant proportion of requests for medical assistance with dying are rejected as unjustifiable, and that the Dutch public have regularly reaffirmed their support for the agreed procedures suggests that, contrary to the claims of some critics, the legalization of voluntary euthanasia has not increased the incidence of non-voluntary euthanasia. A similar picture to the one in the Netherlands has emerged from studies of the operation of the law concerning physician-assisted suicide in Oregon. Indeed, in a recent wide-ranging study of attitudes and practices of voluntary euthanasia and physician-assisted suicide covering two continents, a prominent critic of these practices has concluded (in agreement with his co-authors) that little evidence exists of abuse, particularly of the vulnerable (see Emanuel, et al., 2016). Unfortunately, insufficient time has elapsed for appropriate studies to be conducted in the other jurisdictions that have legalized either voluntary euthanasia or physician-assisted suicide (but for some relevant evidence see e.g., White, et al. 2022). Finally, some commentators have pointed out that there may, in reality, be more danger of the line between voluntary and non-voluntary euthanasia being blurred if euthanasia is practised in the absence of legal recognition, since there will, in those circumstances, be neither transparency nor monitoring (which cannot be said of the Netherlands, Belgium, Oregon and so on).
None of this is to suggest that it is not necessary to ensure the presence of safeguards against potential abuse of legally protected voluntary euthanasia. This is particularly important for the protection of those who have become incompetent by the time decisions need to be taken about whether to assist them to die. Furthermore, it is, of course, possible that the reform of any law may have unintended effects. However, if the arguments outlined above are sound (and the experience in the Netherlands, Belgium and Luxembourg, along with the more limited experience in several states in the United States and in Canada, is, for the present, not only the best evidence we have that they are sound, but the only relevant evidence), that does not seem very likely.
It is now well-established in many jurisdictions that competent patients are entitled to make their own decisions about life-sustaining medical treatment. That is why they can refuse such treatment even when doing so is tantamount to deciding to end their life. It is plausible to think that the fundamental basis of the right to decide about life-sustaining treatment – respect for a person’s autonomy and her assessment of what will best serve her well-being – has direct relevance to the legalization of voluntary euthanasia (see, e.g., Dworkin 1998; Young 2007, 2017; Sumner 2011, 2017). In consequence, extending the right of self-determination to cover cases of voluntary euthanasia does not require a dramatic shift in legal policy. Nor do any novel legal values or principles need to be invoked. Indeed, the fact that suicide and attempted suicide are no longer criminal offences in many jurisdictions indicates that the central importance of individual self-determination in a closely analogous context has been accepted. The fact that voluntary euthanasia and physician-assisted suicide have not been more widely decriminalized is perhaps best explained along a similar line to the one that has frequently been offered for excluding the consent of the victim as a justification for an act of killing, namely the difficulties thought to exist in establishing the genuineness of the consent. But, the establishment of suitable procedures for giving consent to voluntary euthanasia and physician-assisted suicide is surely no harder than establishing procedures for competently refusing burdensome or otherwise unwanted medical treatment. The latter has already been accomplished in many jurisdictions, so the former should be achievable as well.
Suppose that the moral case for legalizing voluntary euthanasia and physician-assisted suicide does come to be judged more widely as stronger than the case against legalization, and they are made legally permissible in more jurisdictions than at present. Should doctors take part in the practice? Should only doctors perform voluntary euthanasia? These questions ought to be answered in light of the best understanding of what it is to provide medical care. The proper administration of medical care should promote the welfare of patients while respecting their individual self-determination. It is these twin values that should guide medical care, not the preservation of life at all costs, or the preservation of life without regard to whether patients want their lives prolonged should they judge that life is no longer of benefit or value to them. Many doctors in those jurisdictions where medically assisted death has been legalized and, to judge from available survey evidence, in other liberal democracies as well, see the practice of voluntary euthanasia and physician-assisted suicide as not only compatible with their professional commitments but also with their conception of the best medical care for the dying. That being so, doctors of the same conviction in jurisdictions in which voluntary medically assisted death is currently illegal should no longer be prohibited by law from lending their professional assistance to competent terminally ill persons who request assistance with dying because of irremediable suffering or because their lives no longer have value for them.
- Asscher, E. and S. van de Vathorst, 2020, “First Prosecution of a Dutch Doctor Since the Euthanasia Act of 2002: What Does It Mean?”, Journal of Medical Ethics , 46: 71–75.
- Beauchamp, T. and A. Davidson, 1979, “The Definition of Euthanasia”, The Journal of Medicine and Philosophy , 4: 294–312.
- Bernat, J., B. Gert, and R. Mognielnicki, 1993, “Patient Refusal of Hydration and Nutrition: An Alternative to Physician Assisted Suicide or Voluntary Euthanasia”, Archives of Internal Medicine , 153: 2723–2728.
- Biggar, N., 2004, Aiming to Kill: The Ethics of Suicide and Euthanasia , London: Darton, Longman and Todd.
- Bradley, B., 2009, Well-Being and Death , Oxford: Clarendon Press.
- Braun, E., 2023, “An autonomy-based approach to assisted suicide: a way to avoid the expressivist objection against assisted dying laws”, Journal of Medical Ethics , 49: 497–501.
- Brock, D., 1993, “Voluntary Active Euthanasia”, Hastings Center Report , 22(2): 10–22.
- Burleigh, M., 1994, Death and Deliverance: Euthanasia in Germany c. 1900–1945 , Cambridge: Cambridge University Press.
- Cavanaugh, T., 2006, Double-Effect Reasoning: Doing Good and Avoiding Evil , Oxford: Clarendon Press.
- Commission on the Study of Medical Practice Concerning Euthanasia: Medical Decisions Concerning the End of Life , The Hague: SdU, 1991. (This is known as ‘The Remmelink Report’.)
- Downie, J. and U. Schuklenk, 2021, “Social determinants of health and slippery slopes in assisted dying debates: lessons from Canada”, Journal of Medical Ethics , 47: 662–669.
- Dworkin, R., 1993, Life’s Dominion: An Argument About Abortion, Euthanasia, and Individual Freedom , New York: Random House.
- Dworkin, G., 1998, “Public Policy and Physician-Assisted Suicide”, in Dworkin, Frey, & Bok 1998, pp. 64–80.
- Dworkin, G., R. Frey, and S. Bok, 1998, Euthanasia and Physician-Assisted Suicide: For and Against , Cambridge: Cambridge University Press.
- Emanuel, E., 1999, “What Is the Great Benefit of Legalizing Euthanasia or Physician-Assisted Suicide?”, Ethics , 109: 629–642.
- Emanuel, E., B. Onwuteaka-Philipsen, J. Urwin and J. Cohen, 2016, “Attitudes and Practices of Euthanasia and Physician-Assisted Suicide in the United States, Canada and Europe”, Journal of the American Medical Association , 316: 79–90.
- Finnis, J., 1995, “A Philosophical Case Against Euthanasia” in J. Keown (ed.), Euthanasia Examined: Ethical, Clinical and Legal Perspectives , Cambridge: Cambridge University Press.
- Foley, K. and H. Hendin (eds.), 2002, The Case Against Assisted Suicide: For the Right to End-of-Life Care , Baltimore: The Johns Hopkins University Press.
- Foot, P., 1977, “Euthanasia”, Philosophy and Public Affairs , 6: 85–112.
- Ganzini, L., E. Goy and S. Dobscha, 2009, “Oregonians’ Reasons for Requesting Physician Aid in Dying”, Archives of Internal Medicine , 169: 489–492.
- Gorsuch, N., 2006, The Future of Assisted Suicide and Euthanasia , Princeton, New Jersey: Princeton University Press.
- Griffiths, J., A. Bood, and H. Weyers, 1998, Euthanasia and Law in the Netherlands , Amsterdam: Amsterdam University Press.
- Griffiths, J., H. Weyers and M. Adams, 2008, Euthanasia and Law in Europe , Oxford: Hart Publishing.
- Jackson, E. and J. Keown, 2012, Debating Euthanasia , Oxford: Hart Publishing.
- Keown, J., 2018, Euthanasia, Ethics and Public Policy: an argument against legalization , 2nd edition, New York: Cambridge University Press.
- –––, 2022, “The Logical Link Between Voluntary and Non-Voluntary Euthanasia”, Cambridge Law Journal , 81: 84–108.
- Kim, S., R. De Vries and J. Peteet, 2016, “Euthanasia and Assisted Suicide of Patients with Psychiatric Disorders in the Netherlands 2011 to 2014”, Journal of the American Medical Association Psychiatry , 73: 362–368.
- Kuhse, H. and P. Singer, 1985, Should the Baby Live?: The Problem of Handicapped Infants , Oxford: Oxford University Press.
- Lewis, P., 2007, Assisted Dying and Legal Change , Oxford: Oxford University Press.
- Marquet, R., A. Bartelds, G. Visser, P. Spreeuwenberg and L. Peters, 2003, “Twenty Five Years of Requests for Euthanasia and Physician Assisted Suicide in Dutch General Practice: Trend Analysis”, British Medical Journal , 327: 201–202.
- McIntyre, A., 2001, “Doing Away With Double Effect”, Ethics , 111: 219–255.
- McMahan, J., 2002, The Ethics of Killing: Problems at the Margins of Life , New York: Oxford University Press.
- Onwuteaka-Philipsen, B., A. Brinkman-Stoppelenburg, C. Penning, G. Jong-Krul, J. van Delden and A. van der Heide, 2012, “Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990–2010: A repeated cross-sectional survey”, The Lancet , 380: 908–915.
- Rachels, J., 1986, The End of Life: Euthanasia and Morality , Oxford: Oxford University Press.
- Rietjens, J., P. van der Maas, B. Onwuteaka-Philipsen, J. van Delden and A. van der Heide, 2009, “Two Decades of Research on Euthanasia from the Netherlands: What Have We Learnt and What Questions Remain?”, Journal of Bioethical Inquiry , 6: 271–283.
- Savulescu, J., 2014, “A Simple Solution to the Puzzles of End of Life? Voluntary Palliated Starvation”, Journal of Medical Ethics , 40: 110–113.
- Singer, P. 1994, Rethinking Life and Death: The Collapse of Our Traditional Ethics , Melbourne: Text Publishing.
- Stingl, M., (ed.), 2010, The Price of Compassion: Assisted Suicide and Euthanasia , Peterborough, Ontario: Broadview Press.
- Sumner, L., 2011, Assisted Death: A Study in Ethics and Law , Oxford: Oxford University Press.
- –––, 2017, Physician-Assisted Death: What Everyone Needs to Know , New York: Oxford University Press.
- –––, 2020, “Conscientious Refusal to Provide Medically Assisted Dying”, University of Toronto Law Journal , 71: 1–31.
- van der Heide, A., J.van Delden and B. Onwuteaka-Philipsen, 2017, “End-of-Life Decisions in the Netherlands over 25 Years”, New England Journal of Medicine , 377: 492–494.
- Varelius, J., 2014, “Medical Expertise, Existential Suffering and Ending Life”, Journal of Medical Ethics , 40: 104–107.
- Velleman, J., 1999, “A Right of Self-Termination?”, Ethics , 109: 606–628.
- White, B., L. Willmott, K. Del Villar, J. Hewitt, E. Close, L. Greaves, J. Cameron, R. Meehan and J. Downie, 2022, “Who is Eligible for Voluntary Assisted Death?: Nine Medical Conditions Assessed Against Five Legal Frameworks”, University of New South Wales Law Journal , 45: 401–444.
- Wicclair, M., 2011, Conscientious Objection in Health Care: An Ethical Analysis , Cambridge: Cambridge University Press.
- Winkler, E., 1995, “Reflections on the State of Current Debate Over Physician-Assisted Suicide and Euthanasia”, Bioethics , 9: 313–326.
- Woodward, P., (ed.), 2001, The Doctrine of Double Effect: Philosophers Debate a Controversial Moral Principle , Notre Dame, Indiana: University of Notre Dame Press.
- Young, R., 2007, Medically Assisted Death , Cambridge: Cambridge University Press.
- –––, 2017, “An Argument in Favor of the Morality of Voluntary Medically Assisted Death”, in M. Cholbi (ed.), Euthanasia and Assisted Suicide: Global Views on Choosing to End Life , Santa Barbara: Praeger.
How to cite this entry . Preview the PDF version of this entry at the Friends of the SEP Society . Look up topics and thinkers related to this entry at the Internet Philosophy Ontology Project (InPhO). Enhanced bibliography for this entry at PhilPapers , with links to its database.
- Medically Assisted Dying , an annotated bibliography authored by Robert Young (La Trobe University)
- Eight Reasons Not to Legalize Physician Assisted Suicide , by David Albert Jones, online resource at the Anscombe Bioethics Centre website.
advance directives | decision-making capacity | doing vs. allowing harm | double effect, doctrine of
Copyright © 2024 by Robert Young < robert . young @ iinet . net . au >
- Accessibility
Support SEP
Mirror sites.
View this site from another server:
- Info about mirror sites
The Stanford Encyclopedia of Philosophy is copyright © 2024 by The Metaphysics Research Lab , Department of Philosophy, Stanford University
Library of Congress Catalog Data: ISSN 1095-5054
- Harvard Division of Continuing Education
- DCE Theses and Dissertations
- Communities & Collections
- By Issue Date
- FAS Department
- Quick submit
- Waiver Generator
- DASH Stories
- Accessibility
- COVID-related Research
Terms of Use
- Privacy Policy
- By Collections
- By Departments
Euthanasia and the Law: The Rise of Euthanasia and Relationship With Palliative Healthcare
Citable link to this page
Collections.
- DCE Theses and Dissertations [1188]
Contact administrator regarding this item (to report mistakes or request changes)
18 Advantages and Disadvantages of Euthanasia
Euthanasia is a deliberate action that is taken by a physician or another party that knowingly results in the ending of a person’s life. This step is taken under most circumstances to end the persistent suffering that individuals experience because of a terminal illness, genetic disorder, or traumatic event. It is a process that, along with physician-assisted suicide, is against the law in most countries. These actions may even include a jail sentence if an individual is convicted of this practice.
Voters in Oregon approved the Death with Dignity Act in 1994, allowing a doctor to help a patient with a terminal illness find the peace they wanted. Part of this law required that the patient have only six months or fewer to live with their diagnosis. The Supreme Court ruled in 1990 that non-active euthanasia is permissible. Formal ethics committees in hospitals and nursing homes have existed since 1977 to encourage advanced health directives and living wills.
The Netherlands eliminated the criminalization of assisted suicide in 2002, loosening some of their restrictions at the same time euthanasia was approved for the first time in Belgium. Switzerland was one of the first nations to allow the practice, authorizing doctors in 1937 to help patients if ending their life did not provide them with a personal gain.
There are several advantages and disadvantages to consider with euthanasia, especially since it is such an emotive and sometimes controversial topic.
List of the Advantages of Euthanasia
1. We use euthanasia as the last resort when all other options are off the table. The average person or doctor is not going to support the proactive termination of a life when there is no suffering involved. Euthanasia is different than suicide, even though both actions end a life, because the former uses assistance and the latter does not. The goal with this help is to end the suffering of a lengthy death, especially if there is chronic and severe pain included with the process.
People often criticize pet owners for not taking them to the vet to end their suffering when something tragic occurs – even if it is only cancer or old age. When an individual wants to take the same action, then they receive criticism for it. How does that make sense?
2. The right to die should be a personal choice, not one that the government mandates. We have the right to choose numerous paths in life that can take us in a variety of different directions. Most of those actions receive very little, if any, governmental interference. When we start talking about euthanasia, the story becomes very different. There are some spiritual views of suicide that might influence this discussion, along with the personal difficulties that helping someone might cause, but someone with a terminal illness may wish to end their life on their own terms.
Incorporating Death with Dignity laws can help to make this a possibility. The decision remains in the hands of the patient at all times instead of going to a review panel. Then the patient is the one who takes the fatal prescription or starts the needed IV instead of the doctor so that it remains in a person’s control.
3. Doctors have a minimal role in the modern euthanasia process. One of the reasons why society might be against the idea of euthanasia is because of the actions of people like Dr. Jack Kevorkian in the past. Instead of allowing people with no threat of death to take their lives under supervision, the Death with Dignity Acts that have passed across the United States allow for voluntary physician inclusion. Even if you live in a place that allows this process, such as Washington State or Oregon, then you’re not required to perform this action.
Recent statistics show that less than 1% of doctors choose to participate in these programs. About 40% of those who wrote a legal lethal prescription had no knowledge as to whether or not the patient took the medication. That’s very different from Kevorkian, where 60% of his patients were not terminally ill.
4. There is more control over the final decisions in life. Like it or not, the end of a person’s life is the beginning of a financial journey for their loved ones. Debts are not wiped away at death. Your estate becomes responsible to pay off remaining obligations and handle other items of business. It can take years sometimes to settle complex financial issues. When euthanasia is part of the conversation for someone with a terminal illness, then there can be more planning involved to make this transition easier on everyone else.
By having more control over the final decision of life, the emotional and physical toll of an illness can be reduced for everyone involved. It’s not just relief for the person who is suffering. The rest of the family can find peace knowing that there is a planned time to create an end to this situation.
5. Patients can avoid the issue of caregiver guilt with euthanasia. One of the most significant challenges that occur with a terminal diagnosis is the emotions of guilt and shame that a patient has with regards to their caregivers. They begin to feel like a burden on the people they love, creating a reaction that can cause relationship challenges because it is only natural to push people away to help them to avoid pain. Legalizing euthanasia might not be a popular option in some circles, but it can create organization for the transitory time that everyone experiences in a situation such as this one.
By helping someone to find the physical peace they need, there can be a process of emotional healing that can help everyone push through their grief with greater consistency.
6. We use specific legal requirements to eliminate the threat of a mistaken identity. There are two primary concerns that the critics of euthanasia often express: helping an individual die without their permission or targeting an incorrect patient for this process. The states in the U.S. which have a Death with Dignity Act require that patients self-administer their lethal prescription. You must also be of sound mind when making this decision, and the law requires that you make it more than once after a waiting period.
If someone in an altered state or a patient with a mental disability issued a written request for euthanasia, it would be rejected for a lack of competency. Some jurisdictions require the presence of two witnesses as well, and they cannot be a relative or someone who would benefit from an estate inheritance.
7. Only a handful of people who are terminally ill take advantage of euthanasia laws. Whether you’re looking at data from Europe, the United States, or other countries which allow euthanasia in some way, the results are quite consistent. The people who qualify for this program is 0.3% or less of the general population. When you look at this specific group of people with a terminal illness who decide that this is the method they wish to use to end their life, the rate of adoption is typically less than 3%. Critics are often concerned about the idea that more people would choose suicide because of its accessibility, but the data doesn’t back up that idea.
These figures have been consistent since 2002 in the United States when the first Death with Dignity Act actions were taken. The results are similar to what Europe has experienced since the 1990s with their actions in this area as well.
8. Death is still going to happen, one way or the other. Is the way that a person dies really that important to the rest of society? The advantages and disadvantages of euthanasia should be rightfully debated, but it is not our place to dictate an outside sense of morality or ethics on a person who is trying to manage a terminal diagnosis. These people are already working toward an end-of-life scenario. If they decide not to take advantage of this legal process, there is an excellent chance that they will pass away in the near future anyway.
List of the Disadvantages of Euthanasia
1. The prediction of a terminal diagnosis is rarely accurate. During a 2005 study of terminal illness diagnoses by the Mayo Clinic, they found that only 1 in 5 patients received an accurate number. 17% of people who find themselves in this situation live for longer, sometimes much longer, than what the doctor initially recommends. That is why euthanasia encounters such resistance, even when there are legal definitions in place which allow for its use.
If about 1 in 5 people beat their diagnosis, then what else could be possible? It might be unrealistic to expect a medical miracle in every situation, but we should take an open and honest approach to these statistics.
2. There can be issues with consent when looking at euthanasia. The legalization of euthanasia works when a physician is willing to provide this option for their patient. There are times when a doctor is unwilling to provide a lethal prescription for their own ethical reasons, going back to the concept to “do no harm.” There are some in the medical field that believe the quality of death should be just as much a priority as the quality of life, but the idea of trying to recommend this option is something that critics find to b e a possibility in the future.
No one should ever go through a situation where they feel like their doctor is trying to talk them into the euthanasia process. Doctors need the option to get out of this program just as much as a patient deserves a second option.
3. Euthanasia medication doesn’t always deliver on its promised result. The State of Oregon tracked the results of patients who took lethal prescriptions as part of the Death with Dignity Act for two decades, starting in 1998. This data found that seven people regained consciousness after taking the medication, and one person was even alive after the study period still fighting their disease. Another 1,179 people out of 1,857 qualifying patients had a successful result from their encounter with the euthanasia program.
We must remember that the legalization of euthanasia is not a guaranteed outcome. When someone makes this decision and it doesn’t work as intended, it places them and their doctor into an almost impossible situation. Do you continue to treat the disease? Or do you attempt to help that person end their life once again.
4. Euthanasia could allow people to choose death for reasons that go beyond an illness. When surveying individuals who qualify for a euthanasia program, over 90% said that it was their “loss of autonomy” that was driving their decision – not the actual diagnosis of a terminal illness. The survey asked patients to choose any reason that applied, and 90% of people also chose a restriction in their usual activities as a primary factor in their choice.
Only 1 in 4 people who decide to pursue the idea of euthanasia say that pain is an influencing factor in their decision. If patients are using the Death with Dignity Act to have doctors help to end their life because they don’t like their “new normal,” then doesn’t that go against the purpose of this legislation in the first place?
5. Second opinions are not always necessary for euthanasia. The field of medicine is not an exact science, even if we know that there are certain outcomes that are likely in specific circumstances. If you have a bacterial infection, for example, then taking antibiotics should help to clear things up for you. Is that outcome guaranteed? No.
Medical interventions are based on the idea that the benefits which are possible outweigh the potential risks that you face. That is why a second opinion is often recommended when there is a serious diagnosis. Even if there is a consensus in a patient’s condition, there is an unpredictability to the way a person might respond to treatment. “You get surprises because diseases have their own personality, and every once in a while, a disease that’s usually bad behaves in a more indolent fashion,” Dr. David Steinberg, an oncologist at the Lahey Clinic Medical Center, told NBC News.
6. Euthanasia would require a change to the legal and medical statutes in most countries. Although the United States, the Netherlands, and other countries which offer euthanasia at some level would require little in the way of legislation to permit this practice, it would require a complete overhaul of the criminal justice system in others. Even in the U.S., the judicial system has found that an individual does not have a Constitutional right to ask for a prescription that could end their life.
What we do know from the countries which allow euthanasia is that more people are requesting this service without having a terminal illness. Almost 5% of the individuals who die in the Netherlands each year do so because of euthanasia, with over 30% of the requests coming from individuals above the age of 80 without a significant health diagnosis.
7. Some doctors may purposely give out false information. We already know that 1 in 5 people can survive a terminal diagnosis based on length. The University of Chicago also found that doctors sometimes refuse to even offer an estimate if a patient asks them how long they have to live. 2 out of 5 physicians said that they would give an optimistic time that was up to three times longer than what they thought was possible. If we cannot be honest about patient information even with the presence of death with dignity laws, then isn’t it possible that some people could qualify for a program when the reality of their health was a very different story?
8. Most patients do not go through with the process of euthanasia. Only a small group of people decide that ending their life is the right decision to make. About 15% of people who are given a terminal diagnosis even bring up the idea of taking their life through a lethal prescription in the first place. The patients who then follow through with their doctor about this choice is about 2%. When you get to the individuals who actually take the pills so that they can use their local euthanasia laws, that figure drops to less than 1%.
Because there are so few people who take advantage of this option, it could be more beneficial to direct the resources dedicated to euthanasia into other forms of medical research. Although there isn’t a realistic cure for old age, we might come up with a way to stop cancer reliably, manage Alzheimer’s disease with consistency, and find solutions for genetic conditions that can reduce the quality of life for a person.
9. Euthanasia avoids the benefits of palliative care. Instead of trying to improve the life of a patient who has a terminal diagnosis, euthanasia seeks to take what remains of a person’s life away from them. People who specialize in palliative care can benefit from the new social, spiritual, and physical problems they face with their health. It is a benefit that people with a non-fatal diagnosis can use to their advantage as well. Giving up on the hope of life because of a challenging circumstance isn’t the right message for doctors to send to their patients. Suicide is an action that someone can take on their own in most instances if they are of sound mind and body, which means a doctor doesn’t need to be involved in many of these situations.
10. It can result in accidental life termination. In 2018, Dutch doctor Bert Keizer was asked to come to the home of a man dying from lung cancer. When he arrived, there were over 30 people gathered around the man’s bed, all drinking, crying and grieving – but it was boisterous. Then the patient told everyone to calm down, the children were taken from the room, and Keizer gave the man his shot that would end his life.
It’s not a slippery slope argument. The first prosecution for medical malpractice while administering euthanasia occurred in 2018. When the Dutch passed their laws in 2002, there wasn’t a stipulation in place for the patient to be competent at the time of medication administration. There are even instances where parents call in doctors to euthanize their mentally ill children.
Verdict on the Advantages and Disadvantages of Euthanasia
The idea that people should have a way to control their suffering is one that touches each family and individual in some way. No one wants to see someone needlessly suffer. Even though the result likely ends in death, it may be better to find physical peace than to have a few more months on this planet.
Every person’s situation is unique. Trying to force a moral equivalency on someone when those who are taking such an action have no idea about what it means to live in that situation is unacceptable. We should allow people to have an opportunity to end their life if that’s what they want to do.
The advantages and disadvantages of euthanasia must also look at the doctor’s, the patient’s family, and the other people involved with the decision. If someone is mentally fit and wishes to proceed in this manner instead of hoping for a miracle, then this option can help them to make it a reality.
- Skip to primary navigation
- Skip to main content
- Skip to primary sidebar
UPSC Coaching, Study Materials, and Mock Exams
Enroll in ClearIAS UPSC Coaching Join Now Log In
Call us: +91-9605741000
Euthanasia – Arguments in Favour and Against
Last updated on October 17, 2023 by ClearIAS Team

Euthanasia is the deliberate act of ending a person’s life to relieve them of suffering. It is a complex and ethically sensitive topic that has sparked debates and discussions worldwide. There are different forms of euthanasia, and it is regulated differently in various countries.
Euthanasia (“good death”) is the practice of intentionally ending a life to relieve pain and suffering. It is also known as ‘mercy killing’.
In many countries, there is a divisive public controversy over the moral, ethical, and legal issues of euthanasia. Euthanasia is categorized in different ways, which include voluntary, non-voluntary, or involuntary. Euthanasia is also classified into active and passive Euthanasia.
Table of Contents
Voluntary, Non-Voluntary, and Involuntary Euthanasia
- Voluntary euthanasia: It is conducted with the consent of the patient and is termed voluntary euthanasia. Voluntary euthanasia is legal in some countries. Jurisdictions, where euthanasia is legal, include the Netherlands, Colombia, Belgium, and Luxembourg.
- Non-Voluntary euthanasia: It is conducted where the consent of the patient is unavailable and is termed non-voluntary euthanasia. Non-voluntary euthanasia is illegal in all countries. Examples include child euthanasia, which is illegal worldwide but decriminalized under certain specific circumstances in the Netherlands under the Groningen Protocol.
- Involuntary euthanasia: It is conducted against the will of the patient and is termed involuntary euthanasia. Involuntary euthanasia is usually considered murder.
Passive vs Active euthanasia
Voluntary, non-voluntary, and involuntary euthanasia can all be further divided into passive or active variants.
- Passive euthanasia entails the withholding of common treatments, such as antibiotics, necessary for the continuance of life.
- Active euthanasia entails the use of lethal substances or forces, such as administering a lethal injection, to kill and is the most controversial means.
Euthanasia debate

Euthanasia raises profound ethical and moral questions. Supporters argue that it can be a compassionate and dignified way to end suffering, particularly in cases of terminal illness.
Learn more from: ClearIAS Study Materials
Opponents argue that it raises significant ethical concerns, including the potential for abuse, coercion, and mistakes in diagnosing terminal conditions.
Arguments in Favor
Historically, the euthanasia debate has tended to focus on several key concerns. According to euthanasia opponent Ezekiel Emanuel, proponents of euthanasia have presented four main arguments:
- that people have a right to self-determination, and thus should be allowed to choose their fate
- assisting a subject to die might be a better choice than requiring that they continue to suffer
- the distinction between passive euthanasia, which is often permitted, and active euthanasia, which is not substantive (or that the underlying principle–the doctrine of double effect–is unreasonable or unsound);
- permitting euthanasia will not necessarily lead to unacceptable consequences. Pro-euthanasia activists often point to countries like the Netherlands and Belgium, and states like Oregon, where euthanasia has been legalized, to argue that it is mostly unproblematic.
- Constitution of India: ‘Right to life’ is a natural right embodied in Article 21 but euthanasia/suicide is an unnatural termination or extinction of life and, therefore, incompatible and inconsistent with the concept of ‘right to life’. The State must protect life and the physician’s duty to provide care and not to harm patients. Supreme Court in Gian Kaur Case 1996 has held that the right to life under Article 21 does not include the right to die.
- Caregiver’s burden: Right-to-die supporters argue that people who have an incurable, degenerative, disabling, or debilitating condition should be allowed to die in dignity. This argument is further defended by those, who have chronic debilitating illness even though it is not terminal such as severe mental illness. The majority of such petitions are filed by the sufferers or family members or their caretakers. The caregiver’s burden is huge and cuts across various financial, emotional, time, physical, mental, and social domains.
- Refusing care: The right to refuse medical treatment is well recognized in law, including medical treatment that sustains or prolongs life. For example, a patient suffering from blood cancer can refuse treatment or deny feeds through a nasogastric tube. Recognition of the right to refuse treatment gives way to passive euthanasia.
- Encouraging organ transplantation: Mercy killing in terminally ill patients provides an opportunity to advocate for organ donation. This, in turn, will help many patients with organ failure waiting for transplantation. Not only does euthanasia give the ‘Right to die‘ for the terminally ill, but also the ‘Right to life‘ for the organ needy patients.
Arguments against
Emanuel argues that there are four major arguments presented by opponents of euthanasia:
- not all deaths are painful;
- alternatives, such as cessation of active treatment, combined with the use of effective pain relief, are available;
- the distinction between active and passive euthanasia is morally significant; and
- legalizing euthanasia will place society on a slippery slope, which will lead to unacceptable consequences
- Euthanasia weakens society’s respect for the sanctity of life.
- Euthanasia might not be in a person’s best interests, for example, getting old-aged parents killed for property will.
- Belief in God’s miracle of curing the terminally ill.
- The prospect of a discovery of a possible cure for the disease shortly.
- Proper palliative care makes euthanasia unnecessary.
- There is no way of properly regulating euthanasia.
- Allowing euthanasia will lead to less good care for the terminally ill.
- Allowing euthanasia undermines the commitment of doctors and nurses to save lives.
- Euthanasia may become a cost-effective way to treat the terminally ill.
- Allowing euthanasia will discourage the search for new cures and treatments for the terminally ill.
- Euthanasia gives too much power to doctors.
Euthanasia in India
Passive euthanasia is legal in India. On 7 March 2011, the Supreme Court of India legalized passive euthanasia using the withdrawal of life support to patients in a permanent vegetative state. The decision was made as part of the verdict in a case involving Aruna Shanbaug, who had been in a Persistent Vegetative State (PVS) for 42 years until she died in 2015.
The Aruna Shanbaug Case
In March 2011, the Supreme Court of India passed a historic judgment permitting Passive Euthanasia in the country. This judgment was passed after Pinki Virani’s plea to the highest court in December 2009 under the Constitutional provision of “Next Friend”. It’s a landmark law which places the power of choice in the hands of the individual, over government, medical or religious control which sees all suffering as “destiny”. The Supreme Court specified two irreversible conditions to permit Passive Euthanasia Law in its 2011 Law:
- The brain-dead for whom the ventilator can be switched off.
- Those in a Persistent Vegetative State (PVS) for whom the feed can be tapered out and pain-managing palliatives be added, according to laid-down international specifications.
The same judgment law also asked for the scrapping of 309 , the code that penalizes those who survive suicide attempts. In December 2014, the Government of India declared its intention.
PIL filed by Common Cause
However, on 25 February 2014, a three-judge bench of the Supreme Court of India termed the judgment in the Aruna Shanbaug case to be ‘inconsistent in itself’ and referred the issue of euthanasia to its five-judge Constitution bench on a PIL filed by Common Cause , which case is the basis of the current debate.
Then, the CJI referred to an earlier Constitution Bench judgment which, in the Gian Kaur case , “did not express any binding view on the subject of euthanasia; rather it reiterated that the legislature would be the appropriate authority to bring change.” Though that judgment said the right to live with dignity under Article 21 was inclusive of the right to die with dignity, it did not conclude the validity of euthanasia, be it active or passive.
“So, the only judgment that holds the field about euthanasia in India is the ruling in the Aruna Shanbaug case, which upholds the validity of passive euthanasia and lays down an elaborate procedure for executing the same on the wrong premise that the Constitution Bench in Gian Kaur had upheld the same,” the CJI said.
Common Cause Case: In 2018, the Supreme Court issued a significant judgment in the Common Cause case. The court recognized the right to die with dignity as a fundamental right and permitted passive euthanasia. It provided guidelines for the process and conditions under which passive euthanasia could be allowed.
Government’s endorsement of Passive Euthanasia
On December 23, 2014, the Government of India endorsed and re-validated the Passive Euthanasia judgment law in a Press Release, after stating in the Rajya Sabha as follows: The Hon’ble Supreme Court of India, while dismissing the plea for mercy killing in a particular case, laid down comprehensive guidelines to process cases relating to passive euthanasia.
Thereafter, the matter of mercy killing was examined in consultation with the Ministry of Law and Justice and it has been decided that since the Hon’ble Supreme Court has already laid down the guidelines, these should be followed and treated as law in such cases. At present, there is no legislation on this subject and the judgment of the Hon’ble Supreme Court is binding on all.
The court rejected active euthanasia using lethal injection. In the absence of a law regulating euthanasia in India, the court stated that its decision becomes the law of the land until the Indian parliament enacts a suitable law. Active euthanasia, including the administration of lethal compounds to end life, is still illegal in India, and in most countries.
As India had no law about euthanasia, the Supreme Court’s guidelines are law until and unless Parliament passes legislation. The following guidelines were laid down:
- A decision has to be taken to discontinue life support either by the parents the spouse or other close relatives, or in the absence of any of them, such a decision can be taken even by a person or a body of persons acting as a next friend. It can also be taken by the doctors attending the patient. However, the decision should be taken bona fide in the best interest of the patient.
- Even if a decision is taken by the near relatives or doctors or next friend to withdraw life support, such a decision requires approval from the High Court concerned.
- When such an application is filled, the Chief Justice of the High Court should forthwith constitute a Bench of at least two Judges who should decide whether to approve or not. A committee of three reputed doctors to be nominated by the Bench, will report the condition of the patient. Before giving the verdict, a notice regarding the report should be given to the close relatives and the State. After hearing the parties, the High Court can give its verdict.
A law commission had proposed legislation on “passive euthanasia”, it said. According to the Centre, the decision to come out with a bill was taken after considering the directives of the apex court, the law commission’s 241st report, and a private member bill introduced in Parliament in 2014.
The Centre said that initially, a meeting was held under the chairmanship of B.P. Sharma, secretary in the Health and Family Welfare Ministry, on May 22, 2015, to examine the draft of The Medical Treatment of Terminally Ill Patients (Protection of Patients and Medical Practitioners) Bill and the draft of The Euthanasia (Regulation) Bill.
This move to introduce a bill is a welcome step to clear the grey areas in the Euthanasia debate. Students can also link to this issue while answering questions on:
- Judicial activism: SC framing laws when the parliament hasn’t. Just like the Visaka case.
- Ethical dilemma in Paper 4 .
In India, euthanasia has no legal aspect , and there is no penal law yet introduced in the IPC that specifically deals with euthanasia.
- However, the Supreme Court of India legalized passive euthanasia in 2018 with some conditions, allowing patients to withdraw medical support if they go into an irreversible coma.
- Passive euthanasia is a matter of ‘living will’, and an adult in their conscious mind is permitted to refuse medical treatment or voluntarily decide not to take medical treatment to embrace death naturally, under certain conditions.
- Individuals are only allowed to draft a living will while in a normal state of health and mind.
- Active euthanasia remains illegal in India.
Article by: Jishnu J Raju

Take a Test: Analyse Your Progress
Aim IAS, IPS, or IFS?

About ClearIAS Team
ClearIAS is one of the most trusted learning platforms in India for UPSC preparation. Around 1 million aspirants learn from the ClearIAS every month.
Our courses and training methods are different from traditional coaching. We give special emphasis on smart work and personal mentorship. Many UPSC toppers thank ClearIAS for our role in their success.
Download the ClearIAS mobile apps now to supplement your self-study efforts with ClearIAS smart-study training.
Reader Interactions
February 11, 2016 at 3:48 pm
excellent one..
February 24, 2016 at 8:34 pm
Giving passive euthanasia to a patient who is already dead (not literally) is a right choice.Its better than making them as well as others to suffer.
July 20, 2017 at 4:28 pm
so very true.
July 1, 2016 at 10:58 pm
If the patient does not wants to suffer and himself asking for euthanasia then voluntary euthanasia should be made legal because it will be difficult for him to live than to die. But in case of involuntary euthanasia, there should be some specific time limit upto which the patient’s relatives must wait for him to recover but if there is no improvement like in case of coma , after 7-10 years , there is less chances of the patient to recover. In such cases , involuntary euthanasia should be made legal.
March 16, 2017 at 12:37 pm
no it is not possible If the patient tends to recover over a period of time or suddenly he becomes normal then the involuntary euthanasia will become very dangerous
March 16, 2017 at 12:35 pm
Very Very Useful
June 26, 2018 at 8:12 am
Helpful source I can use to rely on research. Thank you so much, clear IAS.
May 17, 2019 at 9:58 pm
Thanku for quality content
May 23, 2020 at 10:27 pm
“Mercy Killing ” is a responsible debate . It mainly depends on persons will on his /her life.
July 2, 2020 at 2:26 pm
Euthanasia should not be accepted as there is always some hope for better.
May 24, 2021 at 11:57 am
If under Article 21 of the constitution, right to live with dignity is inclusive of right to die with dignity, then why should the provisions under the Euthanasia act be restricted to the old and dying patients. There are a lot of people in their 60s and 70s with limited financial resources, who feel neglected / unwanted by the family who would like to die with dignity rather than be dependent on their children or the other members of family. They may be in good health but would still like to self determine to end their life with dignity. In such cases the law should allow for such people to adopt active Euthanasia. Such people could be persuaded to donate their organs which will help save other lives.
August 25, 2021 at 9:40 am
euthanasia cannot be legalised because of its higher probability of misuse. whether it is for property, money or because of any family problem
August 4, 2022 at 12:11 pm
A thought for all: If you do not have a choice to life, i.e. choose to be born then how can choosing your own means of death, be fair or valid? Something you cannot create or re-created is not yours to manage. My say: God is the giver of life and He alone should take it. Our sufferings are a means of learning, loving, understanding and above all our closeness to Almighty God.
June 28, 2023 at 6:36 pm
ur death is already written whether you take it or god does so doesnt matter
September 19, 2022 at 12:47 pm
I can’t put my dog to sleep for I am as old as he; and despite our handicaps he also wants to live like me.
Boghos L. Artinian
Leave a Reply Cancel reply
Your email address will not be published. Required fields are marked *
Don’t lose out without playing the right game!
Follow the ClearIAS Prelims cum Mains (PCM) Integrated Approach.
Join ClearIAS PCM Course Now
UPSC Online Preparation
- Union Public Service Commission (UPSC)
- Indian Administrative Service (IAS)
- Indian Police Service (IPS)
- IAS Exam Eligibility
- UPSC Free Study Materials
- UPSC Exam Guidance
- UPSC Prelims Test Series
- UPSC Syllabus
- UPSC Online
- UPSC Prelims
- UPSC Interview
- UPSC Toppers
- UPSC Previous Year Qns
- UPSC Age Calculator
- UPSC Calendar 2024
- About ClearIAS
- ClearIAS Programs
- ClearIAS Fee Structure
- IAS Coaching
- UPSC Coaching
- UPSC Online Coaching
- ClearIAS Blog
- Important Updates
- Announcements
- Book Review
- ClearIAS App
- Work with us
- Advertise with us
- Privacy Policy
- Terms and Conditions
- Talk to Your Mentor
Featured on

and many more...
158 Euthanasia Topics & Essay Examples
If you’re writing a euthanasia essay, questions and topics on the subject can be tricky to find. Not with our list!
- 📑 Aspects to Cover in a Euthanasia Essay
🏆 Best Euthanasia Essay Examples & Topics
💡 clever euthanasia titles, 🎓 simple & easy euthanasia essay titles, ✅ most interesting euthanasia topics to write about, ❓ euthanasia essay questions.
Our experts have prepared a variety of ideas for your paper or speech. In the article below, find original euthanasia research questions and essay titles. And good luck with your assignment!
📑 Aspects to Cover in an Euthanasia Essay
Euthanasia is the process of intentional life ending. Its goal is to stop patients’ suffering and pain. In today’s world, euthanasia is a debatable topic, and there are many questions about it.
Euthanasia essays can help students to raise awareness of the process and its aspects. That is why it is crucial to research this issue and write papers on it.
You can discuss various problems in your essay on euthanasia, as there is a broad variety of related issues. You can choose the one you are the most concerned about, search for euthanasia essay questions online or consult your professor.
Here are some examples of euthanasia essay topics and titles we can suggest:
- The benefits and disadvantages of a physician-assisted suicide
- Ethical dilemmas associated with euthanasia
- An individual’s right to die
- Euthanasia as one of the most debatable topics in today’s society
- The ethical dilemma around euthanasia
- The ethics associated with voluntary euthanasia
- Can euthanasia be considered murder?
- Euthanasia debate: Should the government legalize this procedure?
- The legality of physician-assisted suicide in today’s society
Once you have selected one of the euthanasia essay titles, you can start working on your paper. Here are some important aspects to cover:
Start from developing a solid euthanasia essay thesis. You should state the main idea of your paper and your primary argument clearly. A thesis statement can look like this: Euthanasia is beneficial for patients because it prevents them from suffering. Euthanasia can be equal to murder.
- Remember to include a definition of euthanasia and related terms, such as physician-assisted suicide. Your audience should understand what you are talking about in the essay.
- Do not forget to include the existing evidence on the issue. For instance, you can research euthanasia in different countries, the debates around its legalization, and all other aspects related to the problem. Support your claims with facts and cite your sources correctly.
- Legal and ethical questions are some of the most significant aspects you should cover in the essay. Discuss the potential benefits and disadvantages of the procedure, as well as its impact on patients’ families and medical professionals.
- If you are writing an opinion paper, do not forget to state your opinion clearly. Include relevant experience, if possible (for example, if you work at a hospital and patients have asked you about the procedure). Have you met people who could have benefited from euthanasia? Include their stories, if applicable.
- Do not forget to cover the legal aspects of euthanasia in your state. Is it legal to perform some form of euthanasia where you live or work? Do you think it is beneficial for the patients?
- Remember to look at the grading rubric to see what other aspects you should cover in your paper. For example, your professor may want you to state a counter-argument and include a refutation paragraph. Make sure that you follow all of your instructor’s requirements.
- If you are not sure that you have covered all the necessary questions related to your issue, check out related articles and analyze the authors’ arguments. Avoid copying other people’s work and only use it as an inspiration.
Please find our free samples below with the best ideas for your work!
- Euthanasia: Advantages and Disadvantages The most heavily criticized of all such similar actions is involuntary euthanasia which bears the brunt of all severe protests against the issue, with involuntary euthanasia being dubbed as the deprivation of an individual of […]
- Arguments in Favor of Euthanasia Due to the sensitivity of the issue, laws that will protect the rights of both the patient and the physicians who practice euthanasia should be put in place.
- Consequentialism: Euthanasia and Physician-Assisted Suicide People against euthanasia view the consequences of legalization as a gateway to other unethical practices being accepted, which is a slippery slope that could lead to adverse consequences to the fundamental principles and values of […]
- Advantages and Disadvantages of Euthanasia in Modern Society In its turn, this points out to the fact that, in the field of health care, the notion of medicinal compassion organically derives out of the notion of scientific progress, and not out of the […]
- An Argument Against Euthanasia 5 Generally, it is contrary to the duty of the subject of euthanasia and that of those who intend to perform the mercy killing to take one’s life based on their own assessment of the […]
- Why Active Euthanasia is Morally Wrong The issue of active euthanasia has come to the attention of the public over the past decades as more people demand for the right to be assisted to die.
- Euthanasia: Legalisation of a Mercy Killing The fact that the minority of countries and only several states in the US accept euthanasia proves that today people are still not ready to accept it as a mercy.
- Legalizing Euthanasia The are supporters of the idea that only God has the right to take human’s life, on the other hand, the sufferings of the person may be unbearable and they may ask for euthanasia to […]
- The Right to Life and Active Euthanasia The god of every individual should be the only one to bring death to a person and no person should have the authority to accept dying no matter the situation he/she is in.
- The Death Definition and the Need for Euthanasia If the concept of the soul is to be believed in, then one’s death is simply a process that detaches the soul from the body.
- Euthanasia as a Polarizing Issue The example of a plethora of countries shows that the inclusion of assisted suicide is not detrimental to the broad society.
- Rachel’s Stance on Euthanasia: Passive and Active Killing Despite the appealing nature of Rachel’s argument, his claims of equity of killing and letting a person die are not ethically right. A major distinction between killing and witnessing death is the level of responsibility […]
- Euthanasia for Terminally Ill People: Pros & Cons Despite the fact that euthanasia causes a lot of controversy, every person should have the right to end suffering. Permission of euthanasia is the realization of a person’s right to dispose of their body.
- Euthanasia: Arguments for and Against If the disease has reduced a person to a vegetative state and deprived them of consciousness, then their life is no longer fully human and therefore is not considered a blessing.
- Analysis of Ethical Dilemma: Euthanasia One of these is the right to live, which includes much more than the ability to simply exist, and suggests an adherence to a minimum of quality and self-determination.
- Euthanasia-Related Ethical and Legal Issues There are no discussions about whether the person has the right to commit suicide or not because most individuals agree that it is the decision of the adult person who can dispose of their life.
- Euthanasia: Legal Prohibitions and Permits In addition, it is necessary to take into account the right of a suffering person to get rid of the suffering of loved ones.
- Euthanasia: Why Is It Such a Big Problem? Thus, according to the utilitarian viewpoint, there is no problem with euthanasia as along as it is better for the patient. Who is it to decide what is better for the patient?
- Euthanasia and Assisted Suicide as a Current Issue in Nursing Nowadays, even in nations where the procedure of euthanasia and assisted suicide has been legal for decades, this topic continues to be controversial due to ethical and policy issues. However, in the light of the […]
- Euthanasia as Self-Termination Velleman believes that a person should not have the right to end their life as it can make other people suffer, but there is an objection to his opinion related to that person’s own pain.
- Euthanasia and Its Main Advantages However, after realizing the condition is untreatable and having the consent of both the sick person and the relatives, undertaking assisted suicide will enable the patient to evade extreme suffering.
- Euthanasia: Nurses’ Attitudes Towards Death The weakest part of the article is that most of the participants did not clearly define the concept of euthanasia, which casts doubt on the reliability of the sampled data.
- Right to Die With Euthanasia Methods The possible answer is to develop the functionality of both ordinary public hospitals and hospices that are located in their departments. In addition, it is critical to specify the desirable methods of euthanasia.
- “Active and Passive Euthanasia” by James Rachels The second issue about euthanasia that Rachels raises is the difference between killing and allowing one to die. For Rachels, it is necessary to emphasize that killing is sometimes even more humane than allowing one […]
- Arguments Against Legalization of Euthanasia Although the PAS/E should be offered voluntarily to a patient, in some cases it is offered in secret by physicians to patients who are perceived to be dying.
- Euthanasia: The Terri Schiavo Case Analysis The long-term judicial resolution of the Terri Schiavo case was related to the bioethical problem of the humanity of euthanasia, which had many opponents and supporters.
- Can Euthanasia Be Considered Ethical Consequently, from this perspective, the act of euthanasia would be regarded as violence to someone else’s life. As a result, euthanasia is likely to be considered unethical from the point of view of any of […]
- “Active and Passive Euthanasia” and “Sexual Morality” According to Scruton, morality is a constraint upon reasons for action and a normal consequence of the possession of a first-person perspective. For Scruton, sexual morality includes the condemnation of lust and perversion that is, […]
- Nursing Role in Euthanasia Decision and Procedures The weakest point is the lack of analysis of other factors’ influence on the process of euthanasia. The researchers discovered that the role of nurses in euthanasia is underestimated.
- Aspects of Nursing and Euthanasia The subject of the research by Monteverde was to ask people who work in the medical sphere and face the necessity for euthanasia, whether they are for or against it, and why.
- Pros and Cons of Euthanasia from an Ethical Perspective Primarily, this is apparent on American soil, in which some states decriminalized euthanasia, although the supreme court maintained that there is no law that legalized the practice nor the ban of the mentioned act.
- Euthanasia in the Context of Christianity The questions addressed in the paper include the notions of fall and resurrection as means of interpreting suffering, the Christian stance on the value of human life and euthanasia, and the discussion of possible solutions […]
- Nursing Practice and Euthanasia’s Ethical Issues Effective healthcare management is the involvement of all stakeholders, such as CMS, and the federal government in the decision-making process to improve the sustainable growth in the effectiveness of Medicaid.
- Counseling on Euthanasia and End-of-Life Decision The immediate dynamic killing is a clinical demonstration coordinated to the hardship of life, while a doctor helped self-destruction is a demonstration of the doctor where he gives the patient a medicament for taking life.
- Euthanasia and Physician-Assisted Suicide Articles According to the methods of application, there are two main types of euthanasia: “active”, which consists in performing certain actions to accelerate the death of a hopelessly ill person, and “passive”, the meaning of which […]
- Legal and Ethical Issues of Euthanasia Davis argues that there exists a challenge on how to establish a consensus in the competing views regarding the desire for patients to have the choice to die with dignity while under pain and distress […]
- Debates on Euthanasia – Opposes the Use Therefore, the legal system should work hand in hand with healthcare shareholders in distinguishing the limits between the patients’ rights and the physicians’ accountability based on the possible life-limiting treatment choices.
- Active Euthanasia: Ethical Dilema In case of active euthanasia, it is the patient who requests the medical practitioner to end his or her life and the former abides by the wish.
- Euthanasia: Every For and Against Jane L Givens and Susan L Mitchell “Concerns about End-of-Life Care and Support for Euthanasia” Journal of Pain and Symptom Management Article in Press FOR The authors state socio-demographic characteristics of the people are the […]
- Pro Euthanasia in the United States The discussions of euthanasia implementation in the United States began in the early 19th century after the development of ether, which was applied to pain-relieving.
- Human Euthanasia Should Be Allowed It is stated that there is a shift in a social attitude towards human euthanasia, where people are beginning to realize that people’s lives are their rights.
- The Euthanasia in Humans The moral and ethical aspects of medical practice include not only the features of interaction with patients and other interested parties but also deeper nuances. In particular, one of the controversial and acute topics is euthanasia and its acceptability from different perspectives, including both patients’ and healthcare employees’ positions. In addition, religious issues are involved, […]
- Euthanasia: Philosophical Issues at Stake in Rodriguez I will argue that the prohibition of euthanasia contradicts utilitarianism and the principle of quality of life in particular, and can hardly be supported by paternalism since the ban does not benefit an individual’s life.
- “Euthanasia Reconsidered” by Deagle In more detail, there is a clearly discernible introduction that provides the background to the topic, introduces the thesis statement, and state the opinion of the author of the topic discussed.
- Euthanasia Movement in Modern America Euthanasia movements in modern America perfected the art of rhetoric in their communication and this worked for them in terms of winning the heart of the public.
- Euthanasia: The Issue of Medical Ethics In this respect, the position of a physician under the strain of extreme circumstances should be weighed about the value of compassion.
- The Dilemma of Euthanasia It is at this point, when it becomes a contention of professional ethics and moral considerations on the part of Jack and his wife on the one hand, and personal choice on the part of […]
- The Problem of Euthanasia in Animal Shelters Animal shelters are forced to euthanize animals for a number of reasons which includes: Lack of funds to treat sick animals, overcrowding as a result of the increased number of animals brought in by owners […]
- David Velleman’s Views on Euthanasia Velleman is correct in his conviction that in this case, the patient’s decision will be the outcome of a federal right to die; the situation with euthanasia is common to that of abortion with the […]
- Euthanasia: Ethical Debates When a patient is in the final stage of life, sometimes, the disease or the conditions of the patient, cause a lot of physical and psychological suffering.
- Euthanasia Moral and Ethical Agitation If grandma were a dog, most all would agree that the only humane option would be to ‘put her to sleep.’ U.S.citizens are guaranteed certain rights but not the right to wouldie with dignity.’ This […]
- Life-Span Development: Terri Schiavo’s Euthanasia Case Euthanasia is the process of stopping the medical maintenance of a patient’s life when the patient/herself does not want to suffer anymore and the doctors are sure that no improvements in the patient’s condition are […]
- Euthanasia and Other Life Termination Options However, there is a strong case for helping terminally ill patients spend the remainder of their lives with care provided by the medical fraternity and with support from the state and insurance companies. And in […]
- The Problem of Euthanasia Nevertheless, we must recognize that the interruption of life, alone or with the help of doctors, is contrary to one of the basic tenets of Christianity: the more people suffer on earth, the easier it […]
- Euthanasia: Allow Them to Be Free From Body Euthanasia, the practice of deliberately bring about an easy, painless, and moderate death to a person who is in the last days of his life and can no more bear the pain of living, has […]
- Palliative Medicine Replacement for Euthanasia Euthanasia is not about helping ill and dying people to end their pain and bring comfort. Euthanasia undermines the core values of life and decreases the motivation to provide care for the dying.
- Euthanasia in Christian Spirituality and Ethics By examining Christian’s views on the fallenness of the world, the hope of resurrection, and the value of a person’s life, one can see that euthanasia is not a morally acceptable option for a Christian […]
- Euthanasia: A Legalized Right to Die Nothing could be further from the intent of those who favor a limited reconsideration of public policy in the areas of assisted suicide and voluntary active euthanasia.
- Euthanasia and Suicide Issues in Christian Ethics Based on the two perceptions of euthanasia, theological and professional, it is valid to say that assisted suicide is probably not the best way out.
- Euthanasia: Morals, Ethics, and the Value of Life James Rachels however disagrees with the position taken by doctors when it comes to active Euthanasia and argues that, given a case where the patient is in intolerable pain and is certain to die in […]
- Euthanasia. Arguments of Opponents The request of the patient to relieve them from Karma and sufferings that is clarification and healing, nobody gives the right to break life of a physical body.
- Attitudes Related to Euthanasia and Physician-Assisted Suicide Among Terminally Ill Patients Consequently, the outlined safeguard becomes the first line of defense in making sure that only the right individuals with chronic and incurable medical conditions benefit from assisted death.
- Active Euthanasia Legalization Controversy While many people present the notions of medical ethics, the right to life, and the availability of palliative care to oppose active euthanasia, there are those who support it since it is evidence-based in nature […]
- Dying With Dignity: Euthanasia Debate On the other hand, the supporters of the law claim that assisted death is not a suicide, and it allows more end-of-life options for terminally ill patients. The majority of people are concerned with control […]
- Euthanasia Legalization as an Unethical Practice The decision to legalize euthanasia is an idea that societies should ignore since it places many global citizens at risk, fails to provide adequate safeguards, diminishes social values, and undermines the teachings of Islam.
- The Ethics of Euthanasia In the analysis of the claims in favor and against euthanasia, the cause and effect relationships between the factors affecting the choice of euthanasia should be established.
- Today’s Moral Issues: Euthanasia To ensure that the right to life is respect, the law was amended to include assisted or aided suicide as a criminal offense.
- Controversial Issues of Euthanasia Decision We now had to make this difficult decision to end his life and relieve him of all the pain that he was undergoing.
- Confronting Physician-Assisted Suicide and Euthanasia It was because of that pain that led my mother and I to bring her to a Chinese holistic healer who treated her with some sort of secret Chinese medical injection.
- Assisted Suicide and Euthanasia Rights in Canada The article asserts that in the year 1993, Rodriquez petitioned in vain to the Supreme Court of Canada to allow her to undertake euthanasia. In the article, the author asserts that, in the year 1993, […]
- Euthanasia: “Being a Burden” by Martin Gunderson As it was implied in the Introduction, in his article, Gunderson argues in favor of the idea that it is utterly inappropriate to even consider the legalization of voluntary euthanasia, due to a number of […]
- Euthanasia: Fighting for the Right Cause Sommerville is a renowned Samuel Gale Professor of Law at the McGill University in Montreal, the Professor in the Faculty of Medicine, and the Founding Director of the Center for Medicine, Ethics, and Law. The […]
- Euthanasia as a Way of Painless Termination of Life The introduction of the Hippocratic School led to the abolishment of the practice. According to the approach, taking human life is unethical and violation of the core right to life.
- Euthanasia and Other Life-Destroying Procedures From this perspective, it is unethical to decide in favor of an end-of-life procedure on the condition that there are at least minimal chances for a patient’s survival.
- Ethics of Euthanasia and Pain-Relieving This leads to the historical argument that voluntary euthanasia is often the beginning of a slippery slope that gives rise to unintentional euthanasia and the murder of people who are unwanted in society.
- Euthanasia Legalization: Public Policy Debates The requirements of physicians to perform euthanasia and consideration of the second opinion eliminate the violation of legal and ethical stipulations, and thus, control the performance of euthanasia in health care environment. Opponents of euthanasia […]
- Euthanasia: Moral Rationalist View Human beings rely on the available evidence to generate beliefs about life and goals that should be attained, and thus the use of reason leads to success in these objectives.
- Euthanasia: Is It Worth the Fuss? In order to grasp the gist of the deliberations in this essay, it is important to first apprehend what the term euthanasia means and bring this meaning in the context of this essay.
- Active and Passive Euthanasia Analysis and Its Concept The issue of morality is one of the things that have to be mentioned when discussing the concept of euthanasia. In this instance, both the patient and the doctor know that there is no cure […]
- Euthanasia in Today’s Society Euthanasia is the deliberate termination of life with the intention of relieving a patient from pain and suffering. If the prognosis of a patient is gloomy, medical care providers may find it more compassionate to […]
- When Ethics and Euthanasia Conflict? The main aim is to reduce the lifetime of a patient who is terminally ill. There is a deep mistrust of the motivations that fuel euthanasia.
- Religions Views on Euthanasia This essay highlights religious thoughts with regard to the whole issue of euthanasia, bringing into focus the extent to which our society has been influenced by courtesy of the Dr.
- Euthanasia as the Key Controversy of the XXI Century The fact that in the present-day society, human life is put at the top of the entire list of values is a major achievement of the civilization and the fact that the current society is […]
- Euthanasia: Is It the Best Solution? In twentieth century, various agencies erupted to address the practice of euthanasia such as Voluntary Euthanasia Legislation Society in 1935, which was advocating for its legalization in London and the National Society for the Legalization […]
- Euthanasia: Right to Live or Right to Die Euthanasia or mercy killing as it is informally referred is the act of ending a person life if it is deemed to be the only way to help a person get out of their suffering.
- A New Fight to Legalize Euthanasia Before settling down on the conclusion of the need to adopt the practice of euthanasia in our state, it is important to visit some basic aspects that are very key in the issue of euthanasia.
- The Morality of Euthanasia In the meantime the medication and the doctors are not trivial anymore in stopping the pain and the victim despite all the sufferings, he or she is in a vegetative state and there is nothing […]
- The Ethics of Active Euthanasia In support of the euthanasia action, the argument is that there are circumstances when the rule of natural life can be violated.
- Is Euthanasia a Morally Wrong Choice for Terminal Patients? It is imperative to note that for both the opponents and proponents of euthanasia, the quality of life is usually the focal point, even though there is no agreement on the criteria of defining quality […]
- Singer’s Views on Voluntary Euthanasia, Non-voluntary Euthanasia, and Involuntary Euthanasia Hence, if a person consciously consents to die, there are no chances for recovery, and killing is the only way to deprive a patient from pain and suffering, euthanasia can be regarded as voluntary.
- Euthanasia and Assisted Suicide The final act that results in the death of the person is however usually performed by the person intending to die after the provision of information, advice and even the ways through which he or […]
- Euthanasia Authorization Debate Euthanasia, which is equivalent to the termination of life, can be equated to a total breach of the principle of the sacredness of life, as well as the breach of the legal right of human […]
- Moral and Ethical Concerns of Euthanasia in Healthcare In the matter of euthanasia, professionals ought to decide between the overall good of the dying patient and that of other stakeholders.
- Good and Harm to Humanity of the Use a Euthanasia An Overview of Euthanasia The meaning of euthanasia has changed over the years from how it was originally construed to what it means to the contemporary world.
- Euthanasia and Meaning of Life The meaning of life is the most general aspect of judging about the requirements that must be set out by laws and people’s morals in regarding to the voluntary or involuntary taking of that life.
- Euthanasia: Your Right to Die? Although both positions can be supported with a lot of arguments, people should change their absolutely negative vision of euthanasia because the right to die with the help of physicians can be considered as one […]
- Euthanasia and Human’s Right to Die Trying to support human life with the help of modern equipment is a good idea, however, not in case there are no chances for a person to live without that equipment.
- Euthanasia Moral Permissibility Secondly, the application of voluntary euthanasia should not be regarded as the only way of reducing the pain that a patient can experience.
- Euthanasia (Mercy Killing) In some circumstances, the family and friends of the patient might request the hospital to terminate the life of the patient without necessarily informing the patient.
- Euthanasian Issues in Modern Society Is it possible to find the relief in the life which is full of pain and agony for those people who suffer from serious diseases and have only a little chance to get rid of […]
- Euthanasia From a Disciple of Jesus Christ in Today’s World Another form of euthanasia is that of Assisted Suicide where the person intending to end his/her life is provided with the necessary guidance, means as well as information as to how to go about the […]
- Euthanasia and Modern Society Towards this end Battin asserts that “the relief of pain of a patient is the least disputed and of the highest priority to the physician” in direct reference to sole and major reason of carrying […]
- Euthanasia: Moral Issues and Clinical Challenges Therefore, any law that rejects euthanasia is a bad one because it denies the patients the right and the liberty to die peacefully.
- Ethical Issues Surrounding the Choice of Euthanasia in the United States
- The Advantages and Disadvantages of the Legalization of Euthanasia
- Confronting Physician-Assisted Suicide and Euthanasia
- The Difference Between Active and Passive Euthanasia
- Euthanasia: Current Policy, Problems, and Solution
- The Permit and Legalization of Euthanasia for the Terminally Ill Patients
- Moral and Religious Differences Between Euthanasia and Suicide
- The Criticisms and Opposition of Euthanasia in Australia
- Assisted Suicide and Euthanasia It Is Not Murder, It Is Mercy
- The Factors That Influence the Legalization of Active and Passive Euthanasia in the United States
- Roman Catholic Church’s Teachings on Abortion and Euthanasia
- The Different Reasons Why People Are Against Euthanasia
- Religious and Ethical Arguments in Favour of Euthanasia
- The Moral and Ethical Views on the Goal of Euthanasia
- Euthanasia and the Role of Politics and Religion
- The Philosophical, Legal, and Medical Issues on Euthanasia
- General Information About Euthanasia and the Legality of Suicide in Australia
- The Nazi Euthanasia Programme Based on Racial Purity Theories
- Dr. Jack Kevorkian’s Role in Physician-Assisted Suicide and Euthanasia
- Utilitarian and Libertarian Views on Euthanasia
- The Moral and Religious Differences, if Any, Between Euthanasia and Suicide
- Biblical World View About the Euthanasia, Suicide, and Capital Punishment
- The Truth About Euthanasia and Assisted Suicide
- Tracing Back the Origins of the Practice of Euthanasia During the Greeks and Roman Times
- The Causes and Effects of Euthanasia and the Moral Right To Die
- The Arguments Against Euthanasia From a Standpoint of a Catholic Christian in the United States of America?
- Why Should Active Euthanasia and Physician-Assisted Suicide Be Legalized?
- What Are the Good and Bad Sides of Euthanasia?
- Do People Have To Commit Suicide by Euthanasia (Suicide by a Doctor)?
- What Is the Difference Between Passive and Active Euthanasia?
- What Are the Social Issues and Ethical Values of Euthanasia?
- What Is the Current Legal Situation Regarding Euthanasia?
- How Does Prohibition of Euthanasia Limit Our Rights?
- What Is the American Medical Association’s Attitude to Euthanasia?
- Can Hegelian Dialectics Justify Euthanasia?
- What Are the Viewpoints and Studies of the Legalization of Euthanasia in the United States?
- Why Does Parenting Make Euthanasia More Acceptable?
- What Are the Negative Arguments Against Euthanasia?
- Voluntary Euthanasia: What’s Right and Wrong?
- Why Can Christians not Accept Euthanasia?
- Can Euthanasia Help the Terminally Ill?
- What Are the Top Ten Reasons for Legalizing Euthanasia?
- Should Non Voluntary Euthanasia Be Legal?
- What Is the Difference Between Doctor-Assisted Suicide and Euthanasia?
- Why Should Euthanasia and Assisted Suicide Be Legalized?
- What’s Wrong With Involuntary Euthanasia?
- Why Are There So Different Views on Abortion and Euthanasia?
- How Would Christians Respond to the Issue of Abortion and Euthanasia?
- What Are the Objections To Legalizing Euthanasia in Hong Kong?
- How Does Euthanasia Devalue Human Life?
- What Are the Views and Arguments About Euthanasia?
- How May the Christian Faith Inform the Debate Over Euthanasia?
- What Does Euthanasia Mean to Society Today?
- What Are the Religious and Ethical Considerations to the Issue of Euthanasia?
- Euthanasia and Assisted Suicide – Who Wants It?
- Chicago (A-D)
- Chicago (N-B)
IvyPanda. (2024, February 28). 158 Euthanasia Topics & Essay Examples. https://ivypanda.com/essays/topic/euthanasia-essay-examples/
"158 Euthanasia Topics & Essay Examples." IvyPanda , 28 Feb. 2024, ivypanda.com/essays/topic/euthanasia-essay-examples/.
IvyPanda . (2024) '158 Euthanasia Topics & Essay Examples'. 28 February.
IvyPanda . 2024. "158 Euthanasia Topics & Essay Examples." February 28, 2024. https://ivypanda.com/essays/topic/euthanasia-essay-examples/.
1. IvyPanda . "158 Euthanasia Topics & Essay Examples." February 28, 2024. https://ivypanda.com/essays/topic/euthanasia-essay-examples/.
Bibliography
IvyPanda . "158 Euthanasia Topics & Essay Examples." February 28, 2024. https://ivypanda.com/essays/topic/euthanasia-essay-examples/.
- Ethical Dilemma Titles
- Meaning of Life Essay Ideas
- Moral Dilemma Paper Topics
- Afterlife Research Topics
- Belief Questions
- Lifespan Development Essay Titles
- Ethics Ideas
- Human Rights Essay Ideas
- Suffering Essay Topics
- Morality Research Ideas
- Death Penalty Questions
- Healthcare Questions
- Suicide Topics
- Constitution Research Ideas
- Social Justice Essay Ideas
The pros and cons of legalising assisted dying
MPs say it is 'increasingly likely' that euthanasia will be legalised in at least one part of the UK
- Newsletter sign up Newsletter

Pro: an end to suffering
Con: losing legal protection, pro: ending 'mercy killings', con: 'slippery slope', pro: shifting opinion, con: religious concerns.
The broadcaster Jonathan Dimbleby has described the criminalisation of assisted dying as "increasingly unbearable" after his younger brother Nicholas died with motor neurone disease.
Calling on all political parties to commit to a free vote in the next parliament to reform legislation on the issue, Dimbleby said the current laws were "as anachronistically cruel as capital punishment", said The Guardian .
His remarks come as a report by MPs on the health and social care select committee said the government must be "actively involved" in discussions about what to do if assisted dying is legalised in at least one jurisdiction of the UK or its crown dependencies, said The Times .
Subscribe to The Week
Escape your echo chamber. Get the facts behind the news, plus analysis from multiple perspectives.

Sign up for The Week's Free Newsletters
From our morning news briefing to a weekly Good News Newsletter, get the best of The Week delivered directly to your inbox.
Otherwise known as euthanasia, assisted dying is a controversial issue for legislatures worldwide, with widely cited arguments both for and against a practice that is legal in some countries while totally taboo in others.
Allowing patients to end their suffering is not only morally justified but also essential to upholding the right to personal and bodily autonomy, advocates argue.
A major parliamentary inquiry set up last year to explore whether assisted dying should be legalised in the UK received tens of thousands of submissions from people facing "uncontrollable" pain and "unbearable suffering", which palliative care alone cannot fix, The Guardian reported.
Paul Lamb, a paralysed former builder from Leeds who died in June 2021, had lost his legal case to challenge UK laws on assisted dying seven months earlier.
"I cannot understand, in a civilised society like ours, why I should be forced to suffer when millions of people around the world already have the choice I asked for," he said in November 2020.
It is currently a criminal offence under the 1961 Suicide Act to help someone take their own life, punishable by up to 14 years in prison.
Some people believe that legalising euthanasia would put too much power in the hands of doctors, who could abuse their position, or relatives.
Rita Marker, executive director of the International Task Force on Euthanasia and Assisted Suicide in the US, has argued: "Euthanasia and assisted suicide are not about the right to die. They are about the right to kill."
The UK's anti-euthanasia Care Not Killing alliance said that the law is also in place to protect the vulnerable "from being pressured into ending their lives".
Making her case against any law change, Ilora Finlay, a crossbench peer and palliative care physician, told the parliamentary inquiry that legalising euthanasia in Britain could result in between 5,800 and 58,000 assisted deaths a year, based on extrapolated data from countries where it is already legal. "Such demand would divert an already stretched workforce of NHS clinicians," she said.
According to Dignity in Dying , 44% of people would break the law and help a loved one to die, risking 14 years in prison.
In 2022 the Crown Prosecution Service (CPS) said it was considering revising its stance on so-called mercy killings so that defendants are less likely to face criminal charges.
"We are not decriminalising any offence," Max Hill, director of public prosecutions and head of the CPS, told the i news site, but in offences "born solely out of compassion", justice can sometimes "be achieved by not prosecuting".
Campaigners claim that UK police are also increasingly turning a blind eye to people travelling to other countries to assist loved ones to end their life.
Opponents argue that normalising euthanasia would be a move towards legalised murder.
This "slippery slope is real", said James Mildred of Care (Christian Action Research and Education), which campaigns against assisted suicide. In a 2018 article in The Economist , Mildred cited "a steady increase year on year in the number of people being killed or helped to commit suicide by their doctors" in countries that have legalised assisted suicide, as the rules are loosened over time.
"Critics say this is happening in Canada," said New Scientist , "with the criteria for assisted dying having expanded once already and a further change planned for next year." Canada, which introduced Medical Assistance in Dying, or MAID, in 2016, has seen the number of people choosing to end their life rise steadily ever since, with MAID deaths comprising 4.1% of all deaths in 2022.
There has been a significant shift in recent years among both the public and professional medical opinion regarding assisted dying for people with a terminal illness.
Polling for The Guardian last August found 65% of people in the UK believe it should become legal for a doctor to assist an adult of sound mind with less than six months to live to voluntarily end their own life, subject to High Court confirmation.
Dignity in Dying claims this number is even higher, and also that 54% of GPs are supportive or neutral to a law change on assisted dying.
Many religious people, especially Catholics, believe that life is the ultimate gift and that taking that away is usurping power that belongs to God only.
In 2020, the Vatican reiterated the Roman Catholic Church's opposition to assisted suicide and euthanasia, describing them as "intrinsically evil" acts "in every situation or circumstance", The New York Times reported.
Sign up for Today's Best Articles in your inbox
A free daily email with the biggest news stories of the day – and the best features from TheWeek.com

Cartoons Friday's cartoons - a deep fake, down to the wire, and more
By The Week US Published 5 April 24

Speed Read Biden threatened to change U.S. policy on Gaza if civilians were not protected
By Peter Weber, The Week US Published 5 April 24

Talking Point Fans of the late singer-songwriter are unimpressed by previews of the upcoming film
By Jamie Timson, The Week UK Published 5 April 24
- Contact Future's experts
- Terms and Conditions
- Privacy Policy
- Cookie Policy
- Advertise With Us
The Week is part of Future plc, an international media group and leading digital publisher. Visit our corporate site . © Future US, Inc. Full 7th Floor, 130 West 42nd Street, New York, NY 10036.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- v.323(7321); 2001 Nov 10
Why active euthanasia and physician assisted suicide should be legalised
Last month Diane Pretty was refused the legal right to choose the circumstances of her own death. 1 She suffers from motor neurone disease and is experiencing the disintegration of her body. She faces a death that she believes will entail indignity and suffering and physically cannot kill herself. The court has denied her request that her husband be allowed to help her. This decision may be consistent with legal precedent but is morally wrong. That is why the law should be changed.
Suppose that Mrs Pretty became permanently and severely incompetent as a result of brain damage and that her life was being sustained by medical technology. If her doctors believed that medical treatment could provide no benefit because of her inability ever to engage in any self directed activity, then legally they could withdraw life sustaining treatments, including hydration and nutrition. 2 In such circumstances they would foresee that she would die as a result of their failure to perform what would ordinarily be their duty to protect life and health. In most other circumstances clinicians are not allowed this discretion to accelerate foreseeable deaths through inaction.
Against the background of the duty to care, the moral and legal status of not saving a life through failing to treat can be the same as actively taking that life. 3 , 4 For example, a doctor who knowingly allows a patient who could be saved to bleed to death in emergency care might be accused of murder. What is deemed to be morally and legally important here is not the emotionally appealing distinction between omission and commission but the justifiability or otherwise of the clinical outcome. Indeed, the distinction between omission and commission may be of little value in some healthcare settings. When doctors turn off ventilators, foreseeing that death will result, it makes little sense to say that they do so passively.
So it is sometimes acceptable for doctors to stop life sustaining treatments when there are grounds for assuming that this is in the best interests of severely incompetent patients. Equally, action and inaction may be deemed morally and legally equivalent in the context of a deliberate failure to carry out the duty of care to save life when clinicians agree that it should be saved. Thus parliament and the courts should take the next step of recognising that this same equivalence should hold when there is clinical agreement that it is in the best interests of some severely incompetent patients to end their life. 5
The most articulate opponents of involuntary passive and active euthanasia accept that there is no moral difference between commission and omission in the medical withdrawal of life sustaining treatment. Nor do they reject the non-provision of life sustaining treatment in principle. However, they do argue that to be acceptable, such non-provision must fulfil two conditions that rule out involuntary euthanasia in practice. 6 , 7
Firstly, for severely incompetent patients the continuation of treatment must be deemed to be of no medical “benefit” or too “burdensome.” However, for opponents of euthanasia such judgments of benefit and burden must not be linked to any claim that the patient's life is no longer worth living. Once it is accepted that doctors should be allowed to make clinical decisions to end life passively on the basis of such claims, active euthanasia in the best interests of such patients would be the next logical step. Secondly, opponents argue that withdrawing treatment for severely incompetent patients must never be done with the intent of causing death—even if death is a foreseeable consequence. It can only be done to relieve suffering. To do otherwise, they claim, would be tantamount to active euthanasia, and this they see as morally wrong. These arguments are unacceptable for two reasons. 8 , 9
On the one hand, we need to ask what makes life sustaining treatment of no benefit or too burdensome if it can achieve its designated aim of saving life. Severely incompetent patients can only be said to be unable to benefit from further life sustaining treatment or to find it too burdensome if—bottom line—they are judged incapable of benefiting from further life itself. Therefore, when the continuation of life sustaining treatment is described as being of no benefit or of too much burden, the clinician must already have decided that the life of the incompetent patient in question is not worth living and therefore not worth prolonging. This is why withdrawal of treatment is deemed to be in the best interest of the patient and consistent with the duty of care to protect this interest.
On the other hand, if death is in the best interests of some patients—if the withdrawal of life sustaining treatment can be said to be of benefit in this case—then death constitutes a moral good for these patients. And if this is so, why is it wrong to intend to bring about this moral good? For example, suppose a doctor refuses to withdraw life support from an incompetent patient when the clinical team agrees it to be appropriate. He does so for no other reason than his realisation that part of his intention is that she dies a quick and painless death. Far from being morally commendable, his refusal should be viewed as incompatible with what is of real moral importance—the best interests of his patient.
Provided the circumstances are clinically warranted, doctors should be able to withdraw life sustaining treatment when they intend to accelerate death as well as to relieve suffering. Morally, the distinction is irrelevant in this particular context. If passively ending the life of severely incompetent patients is legally and professionally acceptable then involuntary active euthanasia should have the same status.
Returning to Mrs Pretty, why should we not also legalise voluntary active euthanasia in light of these arguments? Were she permanently and severely incompetent, we have seen the circumstances in which her doctors would be allowed to end her life passively and should be allowed to do so actively. Therefore, should she not be able to invite them actively to end her life and to advise them about how this should be done? No one has questioned her competence or courage. Yet her own perception of her best interests, and the perception of those who know and love her, have been judicially overruled.
This decision becomes all the more morally questionable when we realise that Mrs Pretty can refuse life sustaining treatment at any time, and her doctors are legally obliged to respect her choice. 10 Some doctors would probably be only too glad to help Mrs Pretty to end her life. This support should be regarded as a moral good instigated in her interests and at her request. It should be legally condoned—either by the interpretation of existing law by a more courageous judiciary or by new legislation.
Finally, if it can be morally right to kill some competent patients at their request, then it must be morally justified to give them the medical wherewithal to kill themselves. It is open to debate whether what Mrs Pretty requires can best be described as voluntary euthanasia or assisted suicide. To provide either of these to appropriate patients who make a competent request represents respect for their autonomy and their desire to die with what they perceive to be dignity.
Of course, any coherent advocate of active euthanasia and physician assisted suicide must take seriously the problem of slippery slopes—of deciding when a request for helping dying is appropriate. Though this may be difficult, it cannot be impossible. The most important question remains: in the face of so much moral right, where is the wrong?
Acknowledgments
The authors acknowledge the advice given by Julie Stone in preparing this manuscript.
- International edition
- Australia edition
- Europe edition

For the sake of all of us, Sonia Sotomayor needs to retire from the US supreme court
She’s been described as the ‘conscience of the supreme court’. That’s why it pains me to write this
F orget Ruth Bader Ginsburg. It is Sonia Sotomayor who is the greatest liberal to sit on the supreme court in my adult lifetime. The first Latina to hold the position of justice, she has blazed a relentlessly progressive trail on the highest bench in the land.
Whether it was her lone dissent in a North Carolina voting rights case in 2016 (“the court’s conclusion … is a fiction”); her ingenious referencing of Ta-Nehisi Coates, James Baldwin and WEB DuBois in another 2016 dissent over unreasonable searches and seizures; or her withering observation at the Dobbs oral argument in 2021 (“Will this institution survive the stench that this creates in the public perception that the constitution and its reading are just political acts?”), Sotomayor has stood head and shoulders above both her liberal and conservative colleagues on the bench for the past 15 years.
And so it is with good reason that she has been called the “conscience of the supreme court” ( the Nation ), “the truth teller of the supreme court” ( New York Times ) and “the real liberal queen of the court” ( Above the Law ).
I happen to agree 100% with all of those descriptions. But – and it pains me to write these words – I also believe it is time for Sotomayor to retire.
Okay, now it is time to remember Ruth Bader Ginsburg. To recall how RBG, who had survived two bouts of cancer, refused to quit the court despite calls to do so from leading liberals during Barack Obama’s second term office. To hark back to her insistence, in multiple interviews, that it was “ misguided ” to insist she retire and that she would only stand down “ when it’s time ”. To recollect how, on her deathbed in 2020, she told her granddaughter that her “most fervent wish is that I will not be replaced until a new president is installed” – and how it made no difference whatsoever! Donald Trump nominated Amy Coney Barrett as RBG’s replacement just eight days after her death, and Senate Republicans confirmed Barrett to RBG’s vacant seat just eight days before election day.
With Joe Biden trailing Trump in several swing states and Democrats also in danger of losing their razor-thin majority in the Senate, are we really prepared for history to repeat itself? Sotomayor will turn 70 in June. Of course, only Sotomayor knows the full status of her health, still it is public knowledge that she has had type 1 diabetes since she was seven ; had paramedics called to her home ; and is the only sitting justice to have, reportedly , traveled with a medic. To be clear: she could easily – and God willing – survive a potential Trump second term and still be dishing out dissents from the bench come 2029.
But why take that risk? Why not retire now? Why not quit the bench at the same age that justices in Belgium, Australia and Japan are forced to do so?
Let’s deal with the three most obvious objections.
First, wouldn’t a replacement for Sotomayor that Senator Joe Manchin has to approve be less progressive, and more centrist, than our sole Latina, super-progressive justice? Perhaps. But, again, consider the alternative. Would we rather Biden replace Sotomayor with a centrist in 2024 … or Trump replace her with a far-right Federalist Society goon in 2025? Or, what if Trump doesn’t win but the Republican party takes control of the Senate and blocks a second-term Biden from replacing her between 2025 and 2028?
Second, is there really any difference between a 6-3 conservative majority on the court and a 7-2 majority? Isn’t all lost already? Not quite. The damage to our democracy from a 7-2 hard-right court would be on a whole other and existential level. Yes, 6-3 has been a disaster for our progressive priorities ( Dobbs! Bruen! Kennedy! ) but there have also been a handful of key 5-4 victories ( Redistricting ! Razor wire at the border ! Ghost guns !) in cases where Roberts plus one other conservative have come over from the dark side. None of that happens in a 7-2 court. The hard-right conservatives win not just most of the time but every single time.
Third, how can anyone on the left dare ask the first, and only, Latina justice to quit the supreme court?
It’s simple. Women in general, and Latinas especially, will suffer most from a 7-2 supreme court. It is because I am so worried about the future of minority rights in this country that I – reluctantly – want Sotomayor to step aside.
This has nothing to do with her race or her gender. Forget RBG (again). Consider Stephen Breyer. You remember Breyer, right? The bookish and bespectacled liberal justice who quit the supreme court in 2022, at the age of 83, in part because of an intense pressure campaign from the left.
The fact that he was a white man didn’t shield him from criticism – or from calls for him to stand down. In 2021, the progressive group Demand Justice sent a billboard truck to circle the supreme court building with the message: “ Breyer, retire .” I joined in, too. “Retire, retire, retire,” I said in a monologue for my Peacock show in 2021. “Or history may end up judging you, Justice Breyer.”
So why is it okay to pressure Breyer to retire but not Sotomayor? This time round, Demand Justice isn’t taking a position on whether an older liberal justice should quit while a Democratic president and Senate can still replace them and, as HuffPost reports, “on the left, there is little open debate about whether she should retire.”
Democrats, it seems, still don’t seem keen on wielding power or influence over the highest court in the nation. In 2013, Barack Obama met with RBG for lunch and tried to nudge her into retiring, but as the New York Times later reported, Obama “did not directly bring up the subject of retirement to Justice Ginsburg”.
Compare and contrast with Donald Trump. The finance journalist David Enrich, in his book Dark Towers, reveals how the Trump family carried out a “ coordinated White House charm offensive ” to persuade Justice Anthony Kennedy to retire in 2018. Trump himself, according to Vanity Fair , “worked for months to assure Kennedy his legacy would be in good hands”.
The offensive was a success. Out went self-styled moderate Kennedy, in came the hard-right political operative Brett Kavanaugh.
If there is to be a change to the supreme court in 2024, Biden and the Senate majority leader, Chuck Schumer, have only a few months left to make it happen. And yet they don’t seem too bothered about Sotomayor’s age or health. Last week, the White House press secretary, Karine Jean-Pierre, called it “a personal decision for her to make”.
A personal decision? The prospect of a 7-2 conservative supreme court, with a far-right Federalist Soceity apparatchik having taken “liberal queen” Sotomayor’s seat on the bench, should fill us all with dread.
Biden, elected Democrats , and liberals and progressives across the board should be both publicly and privately encouraging Sotomayor to consider what she wants her legacy to be, to remember what happened with RBG, and to not take any kind of gamble with the future of our democracy.
If insanity is doing the same thing again and again and expecting different results, then I’m sorry but a liberal supreme court justice about to enter her 70s and refusing to retire on a Democratic president and Democratic Senate’s watch is nothing short of insane.
Mehdi Hasan is the CEO and editor-in-chief of Zeteo
- Sonia Sotomayor
- US politics
- US supreme court
Most viewed
- Share full article
Advertisement
Subscriber-only Newsletter
Ross Douthat
The birth dearth and the smartphone age.

By Ross Douthat
Opinion Columnist
My newsroom colleagues Jason Horowitz and Gaia Pianigiani have a lovely report this week about family-friendly policies in the Italian province of Alto Adige-South Tyrol, which has the highest birthrate of any region in an aging, depopulating Italy.
Their story is a portrait not just of a particular policy matrix but also the culture that policy can help foster. In particular, it highlights the extent to which the province offers not just direct funding for parents — for the family with six kids profiled in the story, that means 200 euros a month for each child until they turn 3, on top of the family benefits offered by Italy’s national government — but also a more comprehensive attempt to build a child-friendly social order. The province’s parents “enjoy discounted nursery schools, baby products, groceries, health care, energy bills, transportation, after-school activities and summer camps.” Teachers are encouraged “to turn their apartments into small nurseries,” workplaces offer breastfeeding breaks, and one workplace lobby is filled with “fliers advertising ‘Welcome Baby’ backpacks loaded with tips for new parents and picture books.”
As a portrait of a family-friendly exception to a larger anti-natal rule, the story dovetails with arguments in a new book from Tim Carney of The Washington Examiner, “ Family Unfriendly : How Our Culture Made Raising Kids Much Harder Than It Needs to Be,” which focuses on the ways that American society conspires to make parenting seem incredibly high-effort, well-nigh impossible.
Some of what Carney describes is a set of habits that’s beyond the reach of policy. (I don’t think there’s much the government can do to persuade parents to “Have Lower Ambitions for Your Kids,” to select one of his more striking chapter titles.) But some of the sense of overwhelmingness that comes with modern parenting seems like it could be mitigated, not just through a once-a-year benefit or tax credit, but also through small consistent signals of support: the family discount on groceries, the convenient in-home child care option, the open play space, the flexible work space.
If the developed world isn’t going to disappear into a gray and underpopulated future, there needs to be some “change in the overall ethos and structure of parenting,” as my Opinion colleague Jessica Grose put it last year, some rewiring of both parental and societal expectations — a rewiring that one Italian province, in my colleagues’ account, seems to have partly achieved.
But emphasize that “partly.” Last week, The Financial Times’s data maven, John Burn-Murdoch, ran a story under the headline “Why family-friendly policies don’t boost birthrates.” That claim seems to conflict with the lessons of Alto Adige-South Tyrol, but really what Burn-Murdoch meant wasn’t that such policies have no effect at all. It’s just that they don’t seem to boost birthrates enough to make up for whatever social and cultural and economic forces keep pushing them below replacement and then even lower still.
And that’s what you see in the Italian example. My colleagues mention that attempts at family-friendly policymaking in the neighboring province of Trentino, which borders Alto Adige-South Tyrol to the south, have been more disappointing: “Its birthrate has nevertheless plunged to 1.36 children per woman,” which is “much closer to the dismal national average.” This is true, but it’s also true that a birthrate of 1.36 is higher than in any other region in Italy.
So Trentino’s efforts are a failure in the sense that they haven’t matched their neighbor’s more impressive results or prevented stark decline. But maybe they’re also a success relative to the no-policy alternative, a case study in how family-friendly efforts make an important difference at the margin even if they can’t simply overcome larger trends.
What might actually overcome those trends? The harsh answer for the moment appears to be, well, nothing. But a more optimistic answer would reach for some larger idea of meaning and mission as the thing that low-birthrate cultures need to somehow recover.
Part of the explanation for the special fecundity of Alto Adige-South Tyrol, my colleagues suggest, lies in its particular heritage as a Germanic enclave absorbed into the Italian republic, which may instill a special interest in its own cultural survival. Likewise, Carney’s book discusses the Israeli exception to the general rule of rich societies having below-replacement birthrates — an exception that includes secular Israelis as well as the ultra-Orthodox and clearly has something to do with a sense of national mission that the Israeli experiment retains. And another new book, “ Hannah’s Children : The Women Quietly Defying the Birth Dearth,” from Catherine Ruth Pakaluk at the Catholic University of America, looks at a different exceptional group, American women having five or more kids, and finds a similar sense of mission, usually religious, as their defining commonality. (I should note that I’ll be moderating a conversation with Pakaluk and Carney at Catholic University in Washington on the evening of April 29.)
How you would translate this sense of mission from the smaller to the larger scale, from small regions and countries and particularly religious cohorts to mass societies, is a question whose lack of obvious answers leads us back to pessimism. At the very least it’s clear that any sweeping kind of fertility recovery would have to defy current expectations and integrate structures of meaning, habits of family formation and modern lifestyles in a way that nobody can quite see coming yet.
Which brings me to smartphones. One of the best reviews of Carney’s book, from Leah Libresco Sargeant in First Things, pairs it with Jonathan Haidt’s “ The Anxious Generation : How the Great Rewiring of Childhood Is Causing an Epidemic of Mental Illness,” about the effect of phones and screens and social media on childhood and adolescence. Carney’s book has a discussion of the screen world’s negative effects on family life, and Haidt’s book offers a portrait of what’s gone wrong with Western childhood in the smartphone age, the loss of independence and unscheduled play and face-to-face interactions between kids, that would be fully at home in “Family Unfriendly.”
Uniting these accounts, Sargeant makes the point that screens have arguably become a substitute for better forms of family friendliness, a way of managing kids in a society that doesn’t want to really deal with all their disruptive energy, their irreducible non-adultness. It’s a new way of making them seen and not heard, or neither seen nor heard: “A child stooped over a phone,” after all, “is quiet, nondisruptive, and doesn’t have to be in public at all.” If screens are possibly making them unhappier, they’re also making them more tractable in a way that substitutes for any larger social transformation that might make them welcome.
We talked about Haidt’s book a bit on our Times Opinion podcast this week , and there’s much more to say about his argument and the critiques that it has generated. But let’s stay with this question of how screens help manage childhood.
All my biases make me agree with the anti-smartphone case, and indeed my strong suspicion is that the culture smartphones create among not just kids but also 20-something adults helps explain the acceleration of the fertility decline in recent years. But because those are my biases, it’s useful to push against them. So consider a different read on Sargeant’s argument: If screens make kids more manageable, shouldn’t they potentially make it easier to have and rear them?
Yes, in this timeline, their use is often intertwined with helicopter parenting and obsessive achievement culture, and may feed into anti-child tendencies in the wider social landscape. But just as a bare fact of parental life, an iPad really can make a long family trip or plane ride much more bearable for a beleaguered mom or dad. A family network of phones really can make it easier to juggle the responsibility for multiple kids and all their play dates and activities. There really are times when it’s OK for kids to be seen but not heard and for streaming entertainment to play a crucial role in letting a parent get dinner on the table.
Likewise for adults and their screens. My phone distracts me from my kids, it sets a bad example for them, but it also makes it possible for me to be present in all kinds of important ways, even when I have work obligations. Remote work seems to make it easier to have kids and to live in houses and neighborhoods that give them space, to escape the potentially fertility-crushing effects of urban density. The internet makes it easier to encourage eccentric childhood interests, to run a home-schooling cooperative, to connect with grandparents in distant states and more.
In our podcast discussion, I was perhaps a bit more optimistic than my co-hosts about our capacity to create a more smartphone-free form of childhood. But I will concede that we are not going to build a smartphone-free society on any non-apocalyptic timeline.
So to imagine a transformed culture that’s friendlier to families and more welcoming to kids is necessarily to imagine one that employs screens in all kinds of ways, but with a mastery over their effects and an intentionality about their uses that we have not yet been able to achieve.
Jonathan Haidt and Tyler Cowen in friendly combat .
Bryan Garsten on liberalism as a refuge .
Jessica Winter on liberalism as a meltdown .
Matthew Rose on the radical right .
Noah Smith on the incentives of euthanasia.
Was the “Seinfeld” finale actually good ?
The library of Nayib Bukele.
This Week in Decadence
— Derek Thompson, “ The True Cost of the Churchgoing Bust ,” The Atlantic (April 3)
… America didn’t simply lose its religion without finding a communal replacement. Just as America’s churches were depopulated, Americans developed a new relationship with a technology that, in many ways, is the diabolical opposite of a religious ritual: the smartphone. As the social psychologist Jonathan Haidt writes in his new book, “The Anxious Generation,” to stare into a piece of glass in our hands is to be removed from our bodies, to float placelessly in a content cosmos, to skim our attention from one piece of ephemera to the next. The internet is timeless in the best and worst of ways — an everything store with no opening or closing times. “In the virtual world, there is no daily, weekly, or annual calendar that structures when people can and cannot do things,” Haidt writes. In other words, digital life is disembodied , asynchronous , shallow and solitary . Religious rituals are the opposite in almost every respect. They put us in our body, Haidt writes, many of them requiring “some kind of movement that marks the activity as devotional.” Christians kneel, Muslims prostrate and Jews daven. Religious ritual also fixes us in time, forcing us to set aside an hour or day for prayer, reflection or separation from daily habit. (It’s no surprise that people describe a scheduled break from their digital devices as a “Sabbath.”) Finally, religious ritual often requires that we make contact with the sacred in the presence of other people, whether in a church, mosque, synagogue or over a dinner-table prayer. In other words, the religious ritual is typically embodied , synchronous , deep and collective . … Finding meaning in the world is hard too; it’s especially difficult if the oldest systems of meaning-making hold less and less appeal. It took decades for Americans to lose religion. It might take decades to understand the entirety of what we lost.
Advertisements for Myself
I will be participating in two debates next week: Arguing the negative for the proposition “ Is Assisted Dying Moral? ” at Stanford University on Tuesday, April 9 at 5 p.m., and moderating a debate on campus free speech amid the Israel-Hamas war, in Cambridge, Mass., on Thursday, April 11 at 7 p.m. Both events are free but require registration.
Ross Douthat has been an Opinion columnist for The Times since 2009. He is the author, most recently, of “The Deep Places: A Memoir of Illness and Discovery.” @ DouthatNYT • Facebook
IMAGES
COMMENTS
1. Legalization. "The right to die should be a matter of personal choice. We are able to choose all kinds of things in life from who we marry to what kind of work we do and I think when one comes to the end of one's life, whether you have a terminal illness or whether you're elderly, you should have a choice about what happens to you….
Besides, it should also tell you the type of essay you are required to write and the scope. 2. Choose a Captivating Topic. After reading the prompt, you are required to frame your euthanasia essay title. Make sure that the title you choose is captivating enough as it invites the audience to read your essay.
The Pros for Right-to-Die Laws. Here are some arguments in favor of giving patients the right to die and protecting healthcare providers who carry out those wishes. Compare these arguments in favor of death with dignity and the right to die against the cons . A patient's death brings him or her the end of pain and suffering.
This highlights the importance of considering why euthanasia should be legal in this essay. Granting patients the autonomy to make this decision would honor their right to choose how they wish to approach their final moments and put an end to their unbearable suffering.
Euthanasia and assisted suicide are two topics discussed throughout history, mainly because they fall within the scope of life as a human right, which has been universally defended for many years [ 1 ]. However, the mean of the word euthanasia as good death generates conflicts at social, moral, and ethical levels.
The word 'Euthanasia' is derived from Greek, 'Eu' meaning 'good' and 'thanatos' meaning 'death', put together it means 'good death'. Euthanasia is defined as the hastening of death of a patient to prevent further sufferings. Active euthanasia refers to the physician deliberate act, usually the administration of lethal ...
The word euthanasia, originated in Greece means a good death 1.Euthanasia encompasses various dimensions, from active (introducing something to cause death) to passive (withholding treatment or supportive measures); voluntary (consent) to involuntary (consent from guardian) and physician assisted (where physician's prescribe the medicine and patient or the third party administers the ...
The Netherlands was the first country to allow legal euthanasia and assisted suicide in 2002, totaling 1.7-2.8% of total deaths. Euthanasia is generally illegal in the United States, but in a nationwide 2017 American poll, 73% of the public were in favor of euthanasia, and 57% said euthanasia is morally acceptable. These numbers are nearly ...
Arguments based on rights. People have an explicit right to die. A separate right to die is not necessary, because our other human rights imply the right to die. Death is a private matter and if ...
As a medical doctor I have, with some worry, followed the assisted dying debate that regularly hits headlines in many parts of the world. The main arguments for legalisation are respecting self-determination and alleviating suffering. Since those arguments appear self-evident, my book Euthanasia and the Ethics of a Doctor's Decisions—An Argument Against Assisted Dying 1 aimed to contribute ...
The entry sets out five conditions often said to be necessary for anyone to be a candidate for legalized voluntary euthanasia (and, with appropriate qualifications, physician-assisted suicide), outlines the moral case advanced by those in favor of legalizing voluntary euthanasia, and discusses the five most important objections made by those who deny that voluntary euthanasia is morally ...
Here Dr Kailash Chand explains the reasons behind his motion for the introduction of new legislation to allow terminally ill people the choice of an assisted death. Kailash Chand. Wed 1 Jul 2009 ...
The question of why it is a problem if a life is terminated prematurely is rarely raised in euthanasia debates, which is surprising, given the existential perspective that is at issue, besides the medical perspective. Aristotle considers death the most fearful thing, since nothing can be good or bad for someone who is dead.
Abstract. Acting as the conductor on the train of impending death, a divisive turn to the left will hasten human pain and end life; while a swerve to the right will prolong human life, but also, extend unbearable human pain and suffering. One could make sound arguments that both of these grim decisions are equally acts of compassion or malice.
April 5, 2021. At a time when so many are dying against their will, it may seem out of sync to discuss the option of having a doctor help people end their lives when they face intolerable ...
Daniel P. Sulmasy, Ilora Finlay, Faith Fitzgerald, Kathleen Foley, Richard Payne, Mark Siegler Physician-Assisted Suicide: Why Neutrality by Organized Medicine Is Neither Neutral Nor Appropriate, Journal of General Internal Medicine 33, no.8 8 (May 2018): 1394-1399.
In the United States, physician-assisted suicide or aid in dying has always been carefully distinguished from euthanasia. Euthanasia, also called mercy killing, refers to the administration of a lethal medication to an incurably suffering patient. It may be voluntary (the patient requests it) or involuntary. Euthanasia is illegal in the United ...
Euthanasia is a deliberate action that is taken by a physician or another party that knowingly results in the ending of a person's life. This step is taken under most circumstances to end the persistent suffering that individuals experience because of a terminal illness, genetic disorder, or traumatic event. It is a process that, along with physician-assisted suicide, is against the law in ...
Euthanasia ("good death") is the practice of intentionally ending a life to relieve pain and suffering. It is also known as 'mercy killing'. In many countries, there is a divisive public controversy over the moral, ethical, and legal issues of euthanasia. Euthanasia is categorized in different ways, which include voluntary, non ...
Introduction. Euthanasia is defined as "the act of deliberately ending a person's life to relieve suffering". People seek euthanasia as it provides a solution to problems that many views as insurmountable; more specifically to deal with "unbearable" suffering that may arise in life, and or death.
Here are some examples of euthanasia essay topics and titles we can suggest: The benefits and disadvantages of a physician-assisted suicide. Ethical dilemmas associated with euthanasia. An individual's right to die. Euthanasia as one of the most debatable topics in today's society.
Con: losing legal protection. It is currently a criminal offence under the 1961 Suicide Act to help someone take their own life, punishable by up to 14 years in prison. Some people believe that ...
Why active euthanasia and physician assisted suicide should be legalised. St Bartholomew′s and Royal London School of Medicine and Dentistry, Queen Mary, University of London, London E1 2AD. Last month Diane Pretty was refused the legal right to choose the circumstances of her own death. 1 She suffers from motor neurone disease and is ...
And so it is with good reason that she has been called the "conscience of the supreme court" (), "the truth teller of the supreme court" (New York Times) and "the real liberal queen of ...
Carney's book has a discussion of the screen world's negative effects on family life, and Haidt's book offers a portrait of what's gone wrong with Western childhood in the smartphone age ...