The Impact of Black Lung and a Methodology for Controlling Respirable Dust
Affiliation.
- 1 Pittsburgh Mining Research Division, National Institute for Occupational Safety and Health, 626 Cochrans Mill Road, Pittsburgh, PA 15236, USA.
- PMID: 33598636
- PMCID: PMC7885287
- DOI: 10.1007/s42461-020-00278-7
Coal workers' pneumoconiosis (CWP), commonly known as black lung, is caused by the inhalation of respirable coal mine dust and is a disabling and potentially fatal lung disease with no cure. Historically, CWP has taken a tremendous human and financial toll in the US coal mining industry. Recent health surveillance data indicates that CWP continues to occur at elevated levels. Respirable coal dust exposure must be controlled to prevent the development of CWP. The Pittsburgh Mining Research Division of the National Institute for Occupational Safety and Health (NIOSH) conducts laboratory and mine-site research to identify control technologies that can be used to successfully reduce respirable dust levels. Various technologies, using multiple methods of control, can be applied in order to reduce dust levels. An overview of CWP's impact and a general methodology for controlling respirable dust in underground coal mines are discussed in this paper.
Keywords: Coal workers’ pneumoconiosis; Engineering controls; Respirable dust; Underground coal mining.

Grants and funding
- CC999999/ImCDC/Intramural CDC HHS/United States
Featured Clinical Reviews
- Screening for Atrial Fibrillation: US Preventive Services Task Force Recommendation Statement JAMA Recommendation Statement January 25, 2022
- Evaluating the Patient With a Pulmonary Nodule: A Review JAMA Review January 18, 2022
- Download PDF
- Share X Facebook Email LinkedIn
- Permissions
Progressive Massive Fibrosis Identified at Federally Funded Black Lung Clinics in the US
- 1 Department of Medicine, University of Virginia, Charlottesville
- 2 School of Public Health, University of Illinois Chicago, Chicago
- 3 Respiratory Health Division, National Institute for Occupational Safety and Health, Morgantown, West Virginia
- 4 Black Lung Clinic, Stone Mountain Health Services, Jonesville, Virginia
- Research Letter Progressive Massive Fibrosis in Coal Miners From 3 Clinics in Virginia David J. Blackley, DrPH; Laura E. Reynolds, MPH, BSN; Connie Short; Ron Carson; Eileen Storey, MD, MPH; Cara N. Halldin, PhD; A. Scott Laney, PhD JAMA
- Medical News & Perspectives Black Lung Resurgence Raises New Challenges for Coal Country Physicians Rebecca Voelker, MSJ JAMA
Progressive massive fibrosis (PMF) is the most severe and disabling form of coal workers’ pneumoconiosis. 1 Between January 2013 and February 2017, 416 cases were identified in miners in 3 federally funded Black Lung Clinics in Virginia (Stone Mountain Health Services [SMHS]). To our knowledge, this is the largest reported cluster of PMF in the scientific literature. 1 In 2019, the Health Resources and Services Administration required patient-level data collection by each of the 15 federally funded Black Lung Clinics (located in 11 states) and established the Black Lung Data and Resource Center to facilitate epidemiologic analyses. 2 We provide an update on the burden of PMF in coal miners served by SMHS and describe PMF cases identified at all other US Black Lung Clinics.
Read More About
Harris DA , Almberg KS , Blackley DJ, et al. Progressive Massive Fibrosis Identified at Federally Funded Black Lung Clinics in the US. JAMA. 2024;331(5):438–440. doi:10.1001/jama.2023.25578
Manage citations:
© 2024
Artificial Intelligence Resource Center
Cardiology in JAMA : Read the Latest
Browse and subscribe to JAMA Network podcasts!
Others Also Liked
Select your interests.
Customize your JAMA Network experience by selecting one or more topics from the list below.
- Academic Medicine
- Acid Base, Electrolytes, Fluids
- Allergy and Clinical Immunology
- American Indian or Alaska Natives
- Anesthesiology
- Anticoagulation
- Art and Images in Psychiatry
- Artificial Intelligence
- Assisted Reproduction
- Bleeding and Transfusion
- Caring for the Critically Ill Patient
- Challenges in Clinical Electrocardiography
- Climate and Health
- Climate Change
- Clinical Challenge
- Clinical Decision Support
- Clinical Implications of Basic Neuroscience
- Clinical Pharmacy and Pharmacology
- Complementary and Alternative Medicine
- Consensus Statements
- Coronavirus (COVID-19)
- Critical Care Medicine
- Cultural Competency
- Dental Medicine
- Dermatology
- Diabetes and Endocrinology
- Diagnostic Test Interpretation
- Drug Development
- Electronic Health Records
- Emergency Medicine
- End of Life, Hospice, Palliative Care
- Environmental Health
- Equity, Diversity, and Inclusion
- Facial Plastic Surgery
- Gastroenterology and Hepatology
- Genetics and Genomics
- Genomics and Precision Health
- Global Health
- Guide to Statistics and Methods
- Hair Disorders
- Health Care Delivery Models
- Health Care Economics, Insurance, Payment
- Health Care Quality
- Health Care Reform
- Health Care Safety
- Health Care Workforce
- Health Disparities
- Health Inequities
- Health Policy
- Health Systems Science
- History of Medicine
- Hypertension
- Images in Neurology
- Implementation Science
- Infectious Diseases
- Innovations in Health Care Delivery
- JAMA Infographic
- Law and Medicine
- Leading Change
- Less is More
- LGBTQIA Medicine
- Lifestyle Behaviors
- Medical Coding
- Medical Devices and Equipment
- Medical Education
- Medical Education and Training
- Medical Journals and Publishing
- Mobile Health and Telemedicine
- Narrative Medicine
- Neuroscience and Psychiatry
- Notable Notes
- Nutrition, Obesity, Exercise
- Obstetrics and Gynecology
- Occupational Health
- Ophthalmology
- Orthopedics
- Otolaryngology
- Pain Medicine
- Palliative Care
- Pathology and Laboratory Medicine
- Patient Care
- Patient Information
- Performance Improvement
- Performance Measures
- Perioperative Care and Consultation
- Pharmacoeconomics
- Pharmacoepidemiology
- Pharmacogenetics
- Pharmacy and Clinical Pharmacology
- Physical Medicine and Rehabilitation
- Physical Therapy
- Physician Leadership
- Population Health
- Primary Care
- Professional Well-being
- Professionalism
- Psychiatry and Behavioral Health
- Public Health
- Pulmonary Medicine
- Regulatory Agencies
- Reproductive Health
- Research, Methods, Statistics
- Resuscitation
- Rheumatology
- Risk Management
- Scientific Discovery and the Future of Medicine
- Shared Decision Making and Communication
- Sleep Medicine
- Sports Medicine
- Stem Cell Transplantation
- Substance Use and Addiction Medicine
- Surgical Innovation
- Surgical Pearls
- Teachable Moment
- Technology and Finance
- The Art of JAMA
- The Arts and Medicine
- The Rational Clinical Examination
- Tobacco and e-Cigarettes
- Translational Medicine
- Trauma and Injury
- Treatment Adherence
- Ultrasonography
- Users' Guide to the Medical Literature
- Vaccination
- Venous Thromboembolism
- Veterans Health
- Women's Health
- Workflow and Process
- Wound Care, Infection, Healing
- Register for email alerts with links to free full-text articles
- Access PDFs of free articles
- Manage your interests
- Save searches and receive search alerts
Your browser is unsupported
We recommend using the latest version of IE11, Edge, Chrome, Firefox or Safari.
School of Public Health
Unearthing pathology of recent rise in black lung disease.

Story text Heading link Copy link

The first new pathology standards for black lung disease in over 50 years were published based on research from the University of Illinois Chicago School of Public Health. The findings will help pathologists diagnose a new, more aggressive form of the condition and may provide public health officials with additional motivation for passing stricter mining regulations.
Rates of coal workers’ pneumoconiosis, the severe respiratory condition popularly known as black lung disease, resurged in the last two decades after a steep decline in the late 20th century. Work from UIC’s Mining Education and Research Center determined that the rise is likely caused by excessive exposure to silica dust in the coal mine atmosphere, compared with the coal dust that historically put miners at risk.
“In the past, these diseases generally took decades to develop, but we’re seeing them developing in much shorter periods of time, and that it’s much more inflammatory and rapidly progressive,” said Dr. Robert Cohen , clinical professor in the UIC School of Public Health and director of the center.
Two recent papers from the center expand upon this link, with both comparing the lungs of miners from the mid-20th century with those from more recent cases of black lung disease. The studies are the first update on the pathology of black lung disease since 1971, highlighting features in lung tissue that are unique to this newer version and making pathologists aware of its changing nature in modern miners.
“In a textbook today, the teaching would be that it would take decades and decades of exposure to develop pneumoconiosis,” said Dr. Leonard Go , research assistant professor and assistant director of center. “But we’re seeing cases of disease in people with five, six years of exposure, sometimes less. And that’s almost certainly because of a more prominent silica component of contribution to their disease.”
Silica dust is known to be highly toxic, causing lung damage, cancer and COPD. While exposure to the substance in most professions is already limited by OSHA regulations, coal miners — governed by a separate federal agency — are still legally allowed to inhale twice as much of the dust on the job. Modern changes in coal mining, such as increased use of heavy machinery and mining of thinner coal seams surrounded by silica, may also contribute to higher exposures, the researchers said.
In one paper , the center researchers conducted a statistical comparison of lung tissue from miners born between 1885 to 1950. The historical samples were gathered from an archive in West Virginia at the Respiratory Health Division of the National Institute for Occupational Safety & Health that the researchers discovered in the basement of the facility.
“It was almost like discovering archaeological evidence, because it has these ancient lungs from guys that were born in the early 20th century,” Cohen said. “It was kind of exciting for us, as pulmonary detectives, to find it.”
Researchers evaluated the specimens for the presence of progressive massive fibrosis, the most severe form of pneumoconiosis. They grouped each case into coal-type, mixed-type and silica-type based on the microscopic characteristics of the lung nodules.
When analyzed over time according to the birth year of the miner, the researchers found that the frequency of coal-type and mixed-type disease declined, likely reflecting the passage of stricter mining regulations. Conversely, rates of silica-type disease stayed constant, even increasing among miners born more recently.
“We saw the rise in disease, and now we can see under a microscope that the pattern of disease is clearly consistent with silica,” Go said. “It’s a smoking gun that something has to change to prevent this disease.”
In a second paper , an international panel of pathologists looked at 85 lung samples, but were not told whether they were from historical miners — those born before 1930 — or contemporary miners born after 1930. Once again, the researchers found that silica-type lesions were more common in contemporary miners than their earlier counterparts.
The analysis also offered detailed descriptions of additional features that are unique to the newer form of the disease, including alveolar proteinosis — a condition previously associated with heavy acute silica exposure but not previously observed in coal miners — and signs of inflammation and fibrosis. It also revealed the startling absence in contemporary miners of coal macules and nodules, once considered a hallmark of black lung disease.
The authors hope that this new information will aid diagnosis of the disease in its new form.
“We want pathologists to recognize this disease, to increase the knowledge and awareness of how this disease looks.” Cohen said. “We’re updating the literature so that pathologists are aware of the rapidly progressive nature and the new signs of disease.”
The authors also hope that the new findings will add more urgency to the debate around further limiting coal miners’ exposure to silica dust and lead to quicker passage of new regulations that further reduce miners’ exposure to dust particles. A federal rule bringing mining restrictions in line with OSHA standards is currently under consideration by the Mine Safety and Health Administration.
“We’re hoping that the studies will add more urgency to this issue and help the agency get this rule out,” Cohen said.
Resurgence of Progressive Massive Fibrosis in Coal Miners — Eastern Kentucky, 2016
Weekly / December 16, 2016 / 65(49);1385–1389
David J. Blackley, DrPH 1 ; James B. Crum, DO 2 ; Cara N. Halldin, PhD 1 ; Eileen Storey, MD 1 ; A. Scott Laney, PhD 1 ( View author affiliations )
What is already known about this topic?
The prevalence of coal workers’ pneumoconiosis fell precipitously after implementation of the Coal Mine Health and Safety Act and reached historic lows in the 1990s, with the most severe form, progressive massive fibrosis (PMF), nearly eradicated. Since that time, increases in the prevalence and severity of coal workers’ pneumoconiosis have occurred, especially in central Appalachia.
What is added by this report?
During January 1, 2015–August 17, 2016, a total of 60 patients identified through a single radiologist’s practice had radiographic findings consistent with PMF; 49 had their radiograph taken during 2016. Surveillance data have indicated a resurgence of PMF in recent years, but the cases described in this report represent a large cluster not discovered through routine surveillance.
What are the implications for public health practice?
Effective dust control, enhanced educational outreach, and improved surveillance are needed to protect the respiratory health of U.S. coal miners.
Coal workers’ pneumoconiosis, also known as “black lung disease,” is an occupational lung disease caused by overexposure to respirable coal mine dust. Inhaled dust leads to inflammation and fibrosis in the lungs, and coal workers’ pneumoconiosis can be a debilitating disease. The Federal Coal Mine Health and Safety Act of 1969 (Coal Act),* amended in 1977, established dust limits for U.S. coal mines and created the National Institute for Occupational Safety and Health (NIOSH)–administered Coal Workers’ Health Surveillance Program with the goal of reducing the incidence of coal workers’ pneumoconiosis and eliminating its most severe form, progressive massive fibrosis (PMF), † which can be lethal. The prevalence of PMF fell sharply after implementation of the Coal Act and reached historic lows in the 1990s, with 31 unique cases identified by the Coal Workers’ Health Surveillance Program during 1990–1999. Since then, a resurgence of the disease has occurred, notably in central Appalachia ( Figure 1 ) ( 1 , 2 ). This report describes a cluster of 60 cases of PMF identified in current and former coal miners at a single eastern Kentucky radiology practice during January 2015–August 2016. This cluster was not discovered through the national surveillance program. This ongoing outbreak highlights an urgent need for effective dust control in coal mines to prevent coal workers’ pneumoconiosis, and for improved surveillance to promptly identify the early stages of the disease and stop its progression to PMF.
On June 9, 2016, a radiologist contacted NIOSH to report a sharp increase during the past 2 years in the number of PMF cases among patients who were coal miners seen at his practice serving the easternmost counties of Kentucky. The radiologist requested assistance in conducting an investigation and developing and implementing interventions to reduce the prevalence of disease in the community. NIOSH personnel traveled to Pike County, Kentucky, to assist with the investigation. A case of practice-identified PMF was defined as an International Labor Office classification of large opacity category A, B, or C pneumoconiosis (PMF) in a current or former coal miner receiving a chest radiograph from a single radiology practice in Pike County, Kentucky, during January 1, 2015–August 17, 2016, with completed radiograph classification and occupational history forms. All radiographic classifications were performed by the reporting radiologist, who is an experienced, board-certified radiologist and a NIOSH-certified B Reader (i.e., a physician certified by NIOSH as proficient in classifying radiographs of pneumoconioses) ( 3 ).
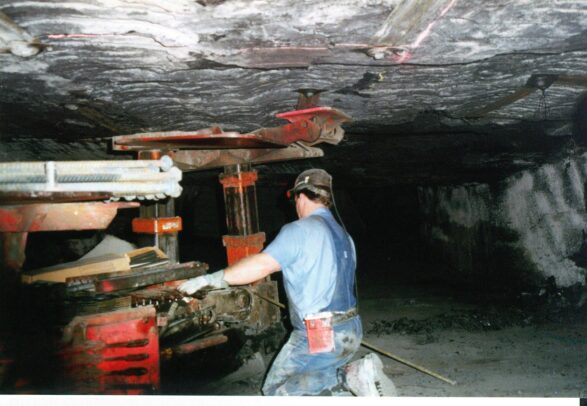
Sixty male patients who were active or former coal miners had radiographic findings consistent with PMF, including 49 (82%) whose radiographs were taken during 2016. Fifty-six (93%) patients were residents of Kentucky; 48 (86%) of the 56 resided in four contiguous counties (Floyd, Knott, Letcher, and Pike) in the southeastern part of the state that are part of the central Appalachian coalfield. The mean age of patients was 60.3 years (range = 44.9–77.4 years; median = 59.4 years). The mean coal mining tenure was 29.2 years (range = 15–47 years; median = 30.0 years). Thirty-one patients (52%) were determined to have category A PMF (one or more large opacities each >10 mm in diameter with combined dimension ≤50 mm); 23 (38%) had category B (combined dimension >50 mm but not exceeding equivalent area of right upper lung zone); and six (10%) had category C (size larger than category B). § All 60 patients had radiographic evidence of pneumoconiosis, including 12 (20%) with a small opacity profusion classified as major category 1, 30 (50%) classified as major category 2, and 18 (30%) classified as major category 3. Seven patients had large, rounded opacities, a finding associated with silicosis lung pathology ( 4 ). Twenty-six patients reported being roof bolters (persons who install the bolts that support the roof of an underground coal mine) for most of their careers, and 20 reported being operators of continuous miners, a type of mining machine that produces a constant flow of coal or other solid material from the working face of the mine ( Figure 2 ).
The voluntary Coal Workers’ Health Surveillance Program stipulates that active coal miners be offered no-cost medical monitoring that includes a chest radiograph at entry into coal mining and then at approximately 5-year intervals. During August 2011–July 2016, a total of 99 unique cases of PMF were detected nationwide by the Coal Workers’ Health Surveillance Program, including 19 in Kentucky residents. Although surveillance data have indicated a resurgence of PMF in recent years (Figure 1), this large cluster of cases brought to the attention of NIOSH by a single local radiologist was not discovered through the national surveillance program offered to active miners. The finding in the current report of 56 cases among Kentucky residents indicates that many cases were not identified through routine national surveillance; however, this finding is consistent with historically low Coal Workers’ Health Surveillance Program participation rates among Kentucky coal miners: during 2011–16 only 17% of Kentucky coal miners participated (personal communication, Coal Workers’ Health Surveillance Program data, October 5, 2016).
The factor or combination of factors that led to this increase in cases of PMF in eastern Kentucky and whether there are more unrecognized cases in neighboring coal mining regions are unknown. Because PMF takes years to become manifest, the specific exposures or mining practices that led to these cases are also unknown. New or modified mining practices in the region might be causing hazardous dust exposures. While obtaining detailed occupational histories, the reporting physician identified the practice of “slope mining” ( 5 ) as a potential exposure in eastern Kentucky (slope mining involves teams of miners operating continuous miner machines, designed to cut coal and other soft rock, to cut shafts through hundreds of feet of sandstone to reach underground coal seams) (Figure 2). The sandstone formation underlying eastern Kentucky is >90% quartz ( 6 ), and dust generated during the slope cutting could expose miners to hazardous dust containing high concentrations of respirable crystalline silica. Previous research found that 25 of 37 (68%) Kentucky and Virginia coal miners with “advanced pneumoconiosis” (defined as PMF or simple coal workers’ pneumoconiosis with high small opacity profusion) reported working as roof bolters, a mining job associated with high silica dust exposure ( 7 ). The current investigation was limited to miners with PMF and found that 26 (43%) reported working as roof bolters, and 20 (33%) reported working as continuous miner operators. Operating a continuous miner machine has typically been considered a “coal-face position” (i.e., a work position located at the face, or seam, of coal), and therefore not a position usually associated with higher silica dust exposures. However, the use of a continuous miner machine during shaft cutting or thin seam coal mining (i.e., occurring when the height of the coal seam requires that rock above and below the coal seam is cut along with the coal) requires cutting through rock and creates the potential for respirable silica exposures, which might explain why working as a continuous miner operator could pose an increased risk for PMF.
In addition, recent industry trends might have led to a higher number of miners seeking radiographs, either to gather information about their health status or to seek benefits through state workers’ compensation or federal black lung programs. A steep decline in coal miner employment and coal production during recent years has occurred ( 8 ), with 1,501 jobs lost in Kentucky (17.9% of state coal workforce) during the first quarter of 2016. Miners might feel that future coal-related employment is unlikely and that previous barriers to health-seeking behaviors have been removed. For example, in Kentucky a miner has 3 years to file a state compensation claim “after the last injurious exposure to the occupational hazard or after the employee first experiences a distinct manifestation of an occupational disease in the form of symptoms reasonably sufficient to apprise the employee that he or she has contracted the disease, whichever shall last occur.” ¶ Because the earlier stages of coal workers’ pneumoconiosis can be associated with few or no overt symptoms, and because coal mining jobs have historically been among the best-paying in the region, some miners might have chosen to not seek radiographs or other health-related information during the earlier stages of their career to avoid threatening their ability to continue working in the industry.
The findings in this report are subject to at least three limitations. First, the cases highlighted in this report represent the recent experience of one single-radiologist practice in eastern Kentucky and might underestimate the actual extent of PMF in coal miners in the broader region. Second, classifications of chest radiographs were performed by a single B Reader, who was aware of miners’ occupational histories and other clinical data, such as results of chest computed tomography scans. For classifications performed for worker monitoring and surveillance, NIOSH recommends that a single reader is generally sufficient, particularly for radiographs that are clearly normal or abnormal. However, for radiographs with findings at the boundary between normal and abnormal, or for settings such as epidemiologic research or contested proceedings where it is important to ensure a high degree of accuracy, NIOSH recommends summary classifications derived from multiple independent readers ( 3 ) and is taking measures to obtain independent confirmation of the classifications by sending them to additional B-readers. Finally, cases in this report were not identified through standard coal workers’ pneumoconiosis surveillance, and whether similar clusters of cases exist in other communities is not known. Thus, the actual extent of PMF in U.S. coal miners remains unclear. Because the cases described in this report were identified during a span of fewer than 2 years and previous radiographs were not available, it was not possible to ascertain the time of PMF onset for these patients.
Although PMF is preventable through well-established dust control practices, each of the 60 patients in this report was exposed to coal mine dust over a period of years in an amount sufficient to cause this severe disease. Finding these cases in such a small geographic area is a strong signal that action is needed in the area to identify existing cases at an earlier stage and prevent future cases. A new federal rule has been implemented to protect all U.S. coal miners through expansion of medical surveillance, including respiratory symptom assessment and spirometry testing ( 9 ). The rule also mandates lowering the amount of respirable dust allowed in U.S. coal mines and the use of a continuous personal dust monitor, a device that can measure respirable coal mine dust in real time. Availability of real-time respirable dust measurements, lower exposure limits, and expanded medical surveillance are intended to prevent future cases and identify early signs of respiratory impairment in coal miners before a disabling condition has developed.
The findings in this report serve as a reminder that more than 45 years after the Coal Act’s passage, one of its core objectives has not been achieved. In the coming years, NIOSH will focus active surveillance measures on miners in central Appalachia and will continue to work with miners, mine operators, regulatory and disability compensation agencies, and others to better characterize the scope of the problem, expand educational outreach to miners to increase their awareness of the right to confidential medical screening, and prevent overexposures to coal mine dust.
Acknowledgments
Heather Wilson, United Medical Group; the NIOSH Coal Workers’ Health Surveillance Program; participating miners.
Corresponding author: David J. Blackley, [email protected] , 304-285-6379.
1 Respiratory Health Division, National Institute for Occupational Safety and Health, CDC; 2 United Medical Group, Pikeville, Kentucky.
* http://arlweb.msha.gov/solicitor/coalact/69act.htm external icon .
† PMF is a fibrotic pneumoconiotic lesion at least 1 cm in diameter; both coal workers’ pneumoconiosis and silicosis can progress to PMF.
§ Radiographs for the pneumoconioses are classified by small opacity profusion and large opacity size, compared with standard radiograph images from the International Labour Office. Large opacities are classified as category A, B, or C. Small opacity profusion is classified into four major categories (0, 1, 2, 3), with category 1 or higher considered to be radiographic evidence of pneumoconiosis ( http://www.cdc.gov/niosh/topics/chestradiography/breader.html ).
¶ http://www.lrc.ky.gov/statutes/statute.aspx?id=32472 external icon .
- Blackley DJ, Halldin CN, Laney AS. Resurgence of a debilitating and entirely preventable respiratory disease among working coal miners. Am J Respir Crit Care Med 2014;190:708–9. CrossRef external icon PubMed external icon
- Laney AS, Weissman DN. Respiratory diseases caused by coal mine dust. J Occup Environ Med 2014;56(Suppl 10):S18–22. CrossRef external icon PubMed external icon
- National Institute for Occupational Safety and Health. Chest radiography. Atlanta, GA: US Department of Health and Human Services, CDC, National Institute for Occupational Safety and Health; 2011. http://www.cdc.gov/niosh/topics/chestradiography/
- Laney AS, Petsonk EL, Attfield MD. Pneumoconiosis among underground bituminous coal miners in the United States: is silicosis becoming more frequent? Occup Environ Med 2010;67:652–6. CrossRef external icon PubMed external icon
- Kentucky Geological Survey. Methods of mining. Lexington, KY: University of Kentucky, Kentucky Geological Survey; 2012. https://www.uky.edu/KGS/coal/coal_mining.htm external icon
- Rice CL. Sandstone units of the Lee Formation and related strata in eastern Kentucky. Professional Paper 1151-G. Washington, DC: US Department of the Interior, US Geological Survey; 1984. https://pubs.usgs.gov/pp/1151g/report.pdf pdf icon external icon
- CDC. Advanced pneumoconiosis among working underground coal miners—Eastern Kentucky and Southwestern Virginia, 2006. MMWR Morb Mortal Wkly Rep 2007;56:652–5. PubMed external icon
- Kentucky Department for Energy Development and Independence. Kentucky Quarterly Coal Report (Q1–2016). Frankfort, KY: Kentucky Department for Energy Development and Independence; 2016. http://energy.ky.gov/Coal%20Facts%20Library/Kentucky%20Quarterly%20Coal%20Report%20(Q1-2016).pdf pdf icon external icon
- Lowering Miners’ Exposure to Respirable Coal Mine Dust, Including Continuous Personal Dust Monitors. 79 FR 24813 (2014). https://www.federalregister.gov/documents/2014/05/01/2014-09084/lowering-miners-exposure-to-respirable-coal-mine-dust-including-continuous-personal-dust-monitors external icon
FIGURE 1 . Prevalence of progressive massive fibrosis (PMF)* among underground-working coal miners with =25 years of underground mining tenure — Coal Workers’ Health Surveillance Program, Kentucky, Virginia, and West Virginia, 1974–2015
Source: Blackley DJ, Halldin CN, Laney AS. Resurgence of a debilitating and entirely preventable respiratory disease among working coal miners. Am J Respir Crit Care Med 2014;190:708–9. Adapted with permission.
* Data are 5-year moving average (e.g., data plotted for 1974 = [PMF 1970 + PMF 1971 + PMF 1972 + PMF 1973 + PMF 1974 ] / [Total participants 1970–1974 ]); surveillance is conducted on a 5-year national cycle.
FIGURE 2 . Photographs of workers and equipment under typical conditions in an underground coal mine*
* A. Two miners use a roof-bolting machine to install the bolts that support the roof of an underground coal mine. B. A continuous miner machine extracts coal from the mine face with a rotating drum.
Suggested citation for this article: Blackley DJ, Crum JB, Halldin CN, Storey E, Laney AS. Resurgence of Progressive Massive Fibrosis in Coal Miners — Eastern Kentucky, 2016. MMWR Morb Mortal Wkly Rep 2016;65:1385–1389. DOI: http://dx.doi.org/10.15585/mmwr.mm6549a1 external icon .
MMWR and Morbidity and Mortality Weekly Report are service marks of the U.S. Department of Health and Human Services. Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services. References to non-CDC sites on the Internet are provided as a service to MMWR readers and do not constitute or imply endorsement of these organizations or their programs by CDC or the U.S. Department of Health and Human Services. CDC is not responsible for the content of pages found at these sites. URL addresses listed in MMWR were current as of the date of publication.
All HTML versions of MMWR articles are generated from final proofs through an automated process. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version ( https://www.cdc.gov/mmwr ) and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
Exit Notification / Disclaimer Policy
- The Centers for Disease Control and Prevention (CDC) cannot attest to the accuracy of a non-federal website.
- Linking to a non-federal website does not constitute an endorsement by CDC or any of its employees of the sponsors or the information and products presented on the website.
- You will be subject to the destination website's privacy policy when you follow the link.
- CDC is not responsible for Section 508 compliance (accessibility) on other federal or private website.
- Official Communications
- Science Sparks
- Current Student Resources
- Faculty and Staff Resources
- Online Learning Resources and Support
- Photography/Video
- Social Media Account Request Form
- UIC Social Media Guidelines and Best Practices
- UIC in the news
- Communicating On Campus
- Sending Announcements / DDDH
- UIC Social Media Directory
Unearthing pathology of recent rise in black lung disease
December 6, 2023
The first new pathology standards for black lung disease in over 50 years were published based on research from the University of Illinois Chicago School of Public Health. The findings will help pathologists diagnose a new, more aggressive form of the condition and may provide public health officials with additional motivation for passing stricter mining regulations.
Rates of coal workers’ pneumoconiosis, the severe respiratory condition popularly known as black lung disease, resurged in the last two decades after a steep decline in the late 20th century. Work from UIC’s Mining Education and Research Center determined that the rise is likely caused by excessive exposure to silica dust in the coal mine atmosphere, compared with the coal dust that historically put miners at risk.
“In the past, these diseases generally took decades to develop, but we’re seeing them developing in much shorter periods of time, and that it’s much more inflammatory and rapidly progressive,” said Dr. Robert Cohen , clinical professor in the UIC School of Public Health and director of the center.
Two recent papers from the center expand upon this link, with both comparing the lungs of miners from the mid-20th century with those from more recent cases of black lung disease. The studies are the first update on the pathology of black lung disease since 1971, highlighting features in lung tissue that are unique to this newer version and making pathologists aware of its changing nature in modern miners.
“In a textbook today, the teaching would be that it would take decades and decades of exposure to develop pneumoconiosis,” said Dr. Leonard Go , research assistant professor and assistant director of center. “But we’re seeing cases of disease in people with five, six years of exposure, sometimes less. And that’s almost certainly because of a more prominent silica component of contribution to their disease.”
Silica dust is known to be highly toxic, causing lung damage, cancer and COPD. While exposure to the substance in most professions is already limited by OSHA regulations, coal miners — governed by a separate federal agency — are still legally allowed to inhale twice as much of the dust on the job. Modern changes in coal mining, such as increased use of heavy machinery and mining of thinner coal seams surrounded by silica, may also contribute to higher exposures, the researchers said.
In one paper , the center researchers conducted a statistical comparison of lung tissue from miners born between 1885 to 1950. The historical samples were gathered from an archive in West Virginia at the Respiratory Health Division of the National Institute for Occupational Safety & Health that the researchers discovered in the basement of the facility.
“It was almost like discovering archaeological evidence, because it has these ancient lungs from guys that were born in the early 20th century,” Cohen said. “It was kind of exciting for us, as pulmonary detectives, to find it.”
Researchers evaluated the specimens for the presence of progressive massive fibrosis, the most severe form of pneumoconiosis. They grouped each case into coal-type, mixed-type and silica-type based on the microscopic characteristics of the lung nodules.

When analyzed over time according to the birth year of the miner, the researchers found that the frequency of coal-type and mixed-type disease declined, likely reflecting the passage of stricter mining regulations. Conversely, rates of silica-type disease stayed constant, even increasing among miners born more recently.
“We saw the rise in disease, and now we can see under a microscope that the pattern of disease is clearly consistent with silica,” Go said. “It’s a smoking gun that something has to change to prevent this disease.”
In a second paper , an international panel of pathologists looked at 85 lung samples, but were not told whether they were from historical miners — those born before 1930 — or contemporary miners born after 1930. Once again, the researchers found that silica-type lesions were more common in contemporary miners than their earlier counterparts.
The analysis also offered detailed descriptions of additional features that are unique to the newer form of the disease, including alveolar proteinosis — a condition previously associated with heavy acute silica exposure but not previously observed in coal miners — and signs of inflammation and fibrosis. It also revealed the startling absence in contemporary miners of coal macules and nodules, once considered a hallmark of black lung disease.
The authors hope that this new information will aid diagnosis of the disease in its new form.
“We want pathologists to recognize this disease, to increase the knowledge and awareness of how this disease looks.” Cohen said. “We’re updating the literature so that pathologists are aware of the rapidly progressive nature and the new signs of disease.”
The authors also hope that the new findings will add more urgency to the debate around further limiting coal miners’ exposure to silica dust and lead to quicker passage of new regulations that further reduce miners’ exposure to dust particles. A federal rule bringing mining restrictions in line with OSHA standards is currently under consideration by the Mine Safety and Health Administration.
“We’re hoping that the studies will add more urgency to this issue and help the agency get this rule out,” Cohen said.

Rob Mitchum [email protected]
Health Sciences Colleges , Research , UIC today
black lung disease , mining , pathology , public health
The Impact of Black Lung and a Methodology for Controlling Respirable Dust
- Published: 30 July 2020
- Volume 37 , pages 1847–1856, ( 2020 )
Cite this article
- Jay F. Colinet 1
437 Accesses
5 Citations
11 Altmetric
Explore all metrics
Coal workers’ pneumoconiosis (CWP), commonly known as black lung, is caused by the inhalation of respirable coal mine dust and is a disabling and potentially fatal lung disease with no cure. Historically, CWP has taken a tremendous human and financial toll in the US coal mining industry. Recent health surveillance data indicates that CWP continues to occur at elevated levels. Respirable coal dust exposure must be controlled to prevent the development of CWP. The Pittsburgh Mining Research Division of the National Institute for Occupational Safety and Health (NIOSH) conducts laboratory and mine-site research to identify control technologies that can be used to successfully reduce respirable dust levels. Various technologies, using multiple methods of control, can be applied in order to reduce dust levels. An overview of CWP’s impact and a general methodology for controlling respirable dust in underground coal mines are discussed in this paper.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions

Similar content being viewed by others

Current Review of Pneumoconiosis Among US Coal Miners
Noemi B. Hall, David J. Blackley, … A. Scott Laney

The Current State of Chinese Coal Mining Dust Hazard and Prevention
NIOSH (1995) Criteria for a recommended standard: occupational exposure to respirable coal mine dust. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, education and information division, DHHS (NIOSH) publication no. 95-106
ILO (2011) Guidelines for the use of the ILO international classification of radiographs of pneumoconioses. International Labour Office, Geneva
Google Scholar
DOL (2019) U.S. Department of Labor, Office of Workers’ Compensation Programs, Division of Coal Mine Workers’ Compensation (DCMWC). https://www.dol.gov/owcp/dcmwc/
NIOSH (2019) Coal workers’ health surveillance program. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, https://www.cdc.gov/niosh/topics/cwhsp/default.html
Code of Federal Regulations (2019) Washington, DC: U.S. Government Printing Office. Office of the Federal Register, Title 30 Part 90, Coal miners who have evidence of the development of pneumoconiosis
NIOSH (2010) Best practices for dust control in coal mining. By Colinet JF, Rider JP, Listak JM, Organiscak JA, Wolfe AL. Pittsburgh, PA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) publication no. 2010-110
79 Federal Register 24814 (2014) Mine Safety and Health Administration: Lowering miners’ exposure to respirable coal mine dust, including continuous personal dust monitors; final rule (to be codified at 30 CFR Parts 70, 71, 72, 75, and 90)
NIOSH (2019) Coal workers’ health surveillance program (CWHSP) data query system. Centers for Disease Control and Prevention. National Institute for Occupational Safety and Health, Respiratory Health Division, Surveillance Branch https://webappa.cdc.gov/ords/cwhsp-database.html
Almberg KS, Halldin CN, Blackley DJ, Laney AS, Storey E, Rose CS, Go LHT, Cohen RA (2018) Progressive massive fibrosis resurgence identified in U.S. coal miners filing for black lung benefits, 1970-2016. Annals American Thoracic Society, 15(12):1420–1426. Data accessed from online supplement: https://www.atsjournals.org/doi/suppl/ https://doi.org/10.1513/AnnalsATS.201804-261OC , Progressive Massive Fibrosis Resurgence Identified in U.S. Coal Miners Filing for Black Lung Benefits, 1970–2016
CDC (2016) Resurgence of progressive massive fibrosis in coal miners – eastern Kentucky, 2016. Morb Mortal Wkly Rep 65(49):1385–1389
Article Google Scholar
Blackley DJ, Reynolds LE, Short C (2018) Progressive massive fibrosis in coal miners from 3 clinics in Virginia. J Am Med Assoc 319(5):500–501
CDC (2019) Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. Occupational Respiratory Disease Surveillance, National Occupational Respiratory Mortality System (NORMS) National Database https://webappa.cdc.gov/ords/norms-national.html
DOL (2019) U.S. Department of Labor, Coal fatalities for 1900 through 2018, Mine Safety and Health Administration. https://arlweb.msha.gov/stats/centurystats/coalstats.asp
DOL (2019) U.S. Department of Labor, Office of Workers’ Compensation Program, Division of Coal Mine Workers’ Compensation (DCMWC), Black Lung Program Statistics, Black lung benefit payment totals by year. https://www.dol.gov/owcp/dcmwc/statistics/TotalBenefitsPayment.htm
Blackley DJ, Halldin CN, Laney AS (2018) Continued increase in lung transplantation for coal workers’ pneumoconiosis in the United States. Am J Ind Med 61(7):621–624
Organiscak JA, Khair AW, Ahmad M (1996) Studies of bit wear and respirable dust generation. Society for Mining, Metallurgy, and Exploration Transactions, Vol 298:1874–1879
USBM (1985) How twelve continuous miner sections keep dust levels at 0.5 mg/m 3 or less. Pittsburgh, PA: U.S. Department of the Interior, U.S. Bureau of Mines, technology news 220
Ludlow J, Jankowski RA (1984) Use lower shearer drum speeds to achieve deeper coal cutting. Min Eng 36(3):251–255
BCR National Laboratory (1985) Dust control handbook for longwall mining operations. U.S. Bureau of Mines contract J0348000. NTIS No. PB 96–178159/AS
Foster-Miller (1990) Evaluate fundamental approaches to longwall dust control; subprogram C – stageloader dust control. U.S. Bureau of Mines contract J03118097. NTIS No. DE 90–015510
Colinet JF, Jankowski RA (2000) Silica collection concerns when using flooded-bed scrubbers. Min Eng 52(4):49–54
Listak JM, Beck TW (2008) Laboratory and field evaluation of dust collector bags for reducing exposure of roof bolter operators. Min Eng 60(7):57–63
Listak JM, Beck TW (2012) Development of a canopy air curtain to reduce roof bolters’ dust exposure. Min Eng 64(7):72–79
Pollock D, Organiscak J (2007) Airborne dust capture and induced airflow of various spray nozzle designs. Aerosol Sci Technol 41(7):711–720
Jankowski RA, Kissell FN, Harrison DJ (1986) Longwall dust control: an overview of progress in recent years. Min Eng 38(10):953–958
USBM (1986) Improved shearer-clearer for longwall dust control. Pittsburgh, PA: U.S. Department of the Interior, U.S. Bureau of Mines, technology news 245
Organiscak J, Beck T (2010) Continuous miner spray considerations for optimizing scrubber performance in exhaust ventilation systems. Min Eng 62(10):41–46
Klima SS, Organiscak JA, Colinet JF (2019) Reducing shuttle car operator dust exposure by improving continuous miner blowing face ventilation parameters. SME annual meeting, Preprint 19–078, February 25–27, 2019
NIOSH (2011) Evaluation of face dust concentrations at mines using deep-cutting practices. By Potts JD, Reed WR, Colinet JF. Pittsburgh, PA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) publication no. 2011-131, RI 9680
NIOSH (2013) Impact on respirable dust levels when operating a flooded-bed scrubber in 20-foot cuts. By Colinet JF, Reed WR, Potts JD. Pittsburgh, PA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) publication no. 2014-105, RI 9693
Ruckley VA, Fernie JM, Chapman JS, Collings P, Davis JMG, Douglas AN, Lamb D, Seaton A (1984) Comparison of radiographic appearances with associated pathology and lung dust content in a group of coal workers. Br J Ind Med 41(4):459–467
Soutar CA, Collins HPR (1984) Classification of progressive massive fibrosis of coalminers by type of radiographic appearance. Br J Ind Med 41(3):334–339
Hall NB, Blackley DJ, Halldin CN, Laney AS (2019) Continued increase in prevalence of r-type opacities among underground coal miners in the USA. Occup Environ Med 76(7):479–481
Castranova V (2000) From coal mine dust to quartz: mechanisms of pulmonary pathogenicity. Inhal Toxicol 12(sup3):7–14
Download references
The findings and conclusions in this report are those of the author and do not necessarily represent the official position of the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention. Mention of any company name, product, or software does not constitute endorsement by NIOSH.
Author information
Authors and affiliations.
Pittsburgh Mining Research Division, National Institute for Occupational Safety and Health, 626 Cochrans Mill Road, Pittsburgh, PA, 15236, USA
Jay F. Colinet
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Jay F. Colinet .
Ethics declarations
Conflict of interest.
The author declares that he has no conflict of interest.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Reprints and permissions
About this article
Colinet, J.F. The Impact of Black Lung and a Methodology for Controlling Respirable Dust. Mining, Metallurgy & Exploration 37 , 1847–1856 (2020). https://doi.org/10.1007/s42461-020-00278-7
Download citation
Received : 15 June 2020
Accepted : 23 July 2020
Published : 30 July 2020
Issue Date : December 2020
DOI : https://doi.org/10.1007/s42461-020-00278-7
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Coal workers’ pneumoconiosis
- Respirable dust
- Engineering controls
- Underground coal mining
- Find a journal
- Publish with us
- Track your research
- Alzheimer's disease & dementia
- Arthritis & Rheumatism
- Attention deficit disorders
- Autism spectrum disorders
- Biomedical technology
- Diseases, Conditions, Syndromes
- Endocrinology & Metabolism
- Gastroenterology
- Gerontology & Geriatrics
- Health informatics
- Inflammatory disorders
- Medical economics
- Medical research
- Medications
- Neuroscience
- Obstetrics & gynaecology
- Oncology & Cancer
- Ophthalmology
- Overweight & Obesity
- Parkinson's & Movement disorders
- Psychology & Psychiatry
- Radiology & Imaging
- Sleep disorders
- Sports medicine & Kinesiology
- Vaccination
- Breast cancer
- Cardiovascular disease
- Chronic obstructive pulmonary disease
- Colon cancer
- Coronary artery disease
- Heart attack
- Heart disease
- High blood pressure
- Kidney disease
- Lung cancer
- Multiple sclerosis
- Myocardial infarction
- Ovarian cancer
- Post traumatic stress disorder
- Rheumatoid arthritis
- Schizophrenia
- Skin cancer
- Type 2 diabetes
- Full List »
share this!
March 26, 2024
This article has been reviewed according to Science X's editorial process and policies . Editors have highlighted the following attributes while ensuring the content's credibility:
fact-checked
peer-reviewed publication
trusted source
Researchers identify protein sensor that plays a role in lung fibrosis
by Weill Cornell Medical College
, the SEL1L protein (tagged green) is prominent. The fibrotic lung tissue (right) is characterized by excess collagen (tagged red), and the SEL1L protein isn't observed suggesting a defective collagen clearing pathway. Credit: Michael J. Podolsky")
Researchers at Weill Cornell Medicine have discovered a protein called SEL1L that plays a critical role in clearing collagen from tissue, and that may be a therapeutic target to help prevent fibrosis, scar tissue that interferes with organ function. The paper, published on Feb. 20 in Nature Communications , provides clues that could lead to drug development for diseases like lung fibrosis which have no therapeutic options currently.
Corresponding author, Dr. Michael J. Podolsky, assistant professor of medicine at Weill Cornell Medicine, led a team that searched the human genome for genes involved in the process that triggers specialized cells to engulf and digest excess collagen from tissue. Cells called fibroblasts and macrophages pick up collagen fragments for degradation in lysosomes, the trash compactors of cells.
Normal lungs continuously synthesize collagen and degrade excess collagen, keeping the two processes precisely balanced to maintain healthy tissue architecture. Even when lungs are injured and the body responds by increasing the rate of collagen production, simultaneously collagen degradation is increased to prevent the formation of permanent scar tissue . However, when the two processes are uncoupled, the result is disease. In pulmonary fibrosis, for instance, collagen degradation does not keep pace with collagen production, resulting in an excess accumulation.
The researchers discovered a mechanism that cells use to detect collagen production internally and regulate clearance of excess collagen in tissues. The protein SEL1L acts as a sensor that responds to collagen production by triggering another protein called MRC2, which is involved in the uptake and disposal of collagen.
This study suggests that a defective collagen clearing pathway based on MRC2 is a key part of the imbalance in fibrotic disease. The data show when SEL1L is overproduced in cells, it leads to increased MRC2 production and thereby prevents the accumulation of collagen. This pathway could eventually be therapeutically targeted to drive increased clearance of collagen to improve fibrosis when it is impaired.
Next, Dr. Podolsky, who is also an attending physician at NewYork Presbyterian/Weill Cornell Medical Center, plans to investigate how SEL1L is impaired in fibrotic human lungs. The lab is also exploring the molecular consequences of MRC2 being inadequately triggered in pulmonary fibrosis.
Explore further
Feedback to editors

Researchers produce grafts that replicate the human ear
3 hours ago

An infamous 'inflammasome'—a rogue protein complex—appears to underlie a rare and disabling autoimmune disorder
19 hours ago

Researchers discover skin biomarkers in infants that predict early development of food allergies
20 hours ago

Veterans help provide greater insight into Klinefelter and Jacobs syndromes

High-resolution images reveal similarities in protein structures between Alzheimer's disease and Down syndrome

How blocking a neural receptor responsible for addiction could reduce alcohol use

Study finds few hospitals promoting potentially predatory medical payment products

COVID-19 research: Study reveals new details about potentially deadly inflammation
21 hours ago

Enhanced melanoma vaccine offers improved survival for men

How music choices can affect productivity
Related stories.

Video: Can collagen supplements help with aging?
Mar 14, 2024

Research discovers disrupted cellular function behind type 2 diabetes in obesity
Feb 2, 2024

How water guides the assembly of collagen, the building block of all humans
Mar 8, 2024

Targeting mechanosensitive protein could treat pulmonary fibrosis, study suggests
Mar 10, 2021

Promising opportunities for treating skin fibrosis
Oct 21, 2021

New window on fibrosis
Aug 9, 2019
Recommended for you

Micro-patterning: A new system to induce alveolar and airway epithelial cells
23 hours ago

Research suggests fine-tuning of specific excitatory synapse traits could lead to new brain disease treatments

Genetic causes of cerebral palsy uncovered through whole-genome sequencing
Mar 29, 2024
Let us know if there is a problem with our content
Use this form if you have come across a typo, inaccuracy or would like to send an edit request for the content on this page. For general inquiries, please use our contact form . For general feedback, use the public comments section below (please adhere to guidelines ).
Please select the most appropriate category to facilitate processing of your request
Thank you for taking time to provide your feedback to the editors.
Your feedback is important to us. However, we do not guarantee individual replies due to the high volume of messages.
E-mail the story
Your email address is used only to let the recipient know who sent the email. Neither your address nor the recipient's address will be used for any other purpose. The information you enter will appear in your e-mail message and is not retained by Medical Xpress in any form.
Newsletter sign up
Get weekly and/or daily updates delivered to your inbox. You can unsubscribe at any time and we'll never share your details to third parties.
More information Privacy policy
Donate and enjoy an ad-free experience
We keep our content available to everyone. Consider supporting Science X's mission by getting a premium account.
E-mail newsletter
Researchers Awarded $14 Million to Better Understand, Treat Genetic Lung Diseases
A team of researchers led by Darrell N. Kotton , MD, the David C. Seldin Professor of Medicine, has been awarded a five-year, $14 million grant from the NIH’s National Heart, Lung, and Blood Institute (NHLBI) for his research, “Developing Pluripotent Stem Cells to Model and Treat Lung Disease.”
Lung diseases, such as those caused by gene mutations, result in significant morbidity and mortality worldwide. The advent of stem cell discoveries and regenerative medicine presents new opportunities to improve the understanding of these diseases and to develop new treatment approaches.
The new award will fund an integrated, multi-investigator program project grant where four interacting labs headed by four physician-scientists, all located in the Center for Regenerative Medicine (CReM) of Boston University and Boston Medical Center, will develop next generation stem cell-based therapies for currently incurable genetic lung diseases affecting children and adults, including childhood and adult interstitial lung diseases, an inherited form of emphysema, cystic fibrosis and primary ciliary dyskinesia.

The four physician-scientists heading each lab include Kotton together with Professor of Medicine, Andrew A. Wilson , MD, Associate Professor of Medicine, Finn Hawkins , MBBCh, and Assistant Professor of Medicine, Kostas Alysandratos , MD, PhD. The four teams have worked closely together for several years on stem cell-based approaches for treating lung disease, including throughout the pandemic when they famously shared their stem cell bank with researchers across the world to develop new models for understanding and treating COVID-19.
“While it is hard to envision a more optimistic time in health-related research, treatments for many devastating lung diseases have not yet been realized, and clinical therapies in many cases still largely focus on treating symptoms,” says Kotton.
For the new project, Kotton and his teams have developed reprogramming methods to generate induced pluripotent stem cells (iPSCs) from patients and have applied these methods to produce the largest known bank of lung disease-specific iPSCs. Having established these stem cell banks and protocols, Kotton now is focused on applying these resources to advance their mechanistic understanding of how gene mutations initiate airway and alveolar epithelial dysfunction resulting in disease. They seek to intervene with precision therapeutics or regenerative cell therapies. According to Kotton, they will focus initially on ameliorating or curing genetic lung diseases of the airway and alveoli, given that their proximal disease-driving gene mutations are well described.
“The researchers on this new project are not new to this mission, for they have worked together for many years in juxtaposed labs, publishing an extensive literature that provides a solid foundation upon which to now launch a concerted effort to move our field from basic discovery to therapeutic development,” said Kotton.
Kotton is an Allen Distinguished Investigator and an elected member of the American Society of Clinical Investigators and Association of American Physicians. He leads a basic research laboratory, continuously funded by the NIH since 2004 and serves on the NHLBI’s Board of External Experts. He is the recipient of the American Thoracic Society’s Recognition Award for Scientific Accomplishments (2018), the AAMC inaugural national Research Resources Sharing Award (2017), the Alpha-1 Foundation’s Researcher of the Year (2013) and Shillelagh (2010) awards, Boston University’s Graduate Medical Sciences Educator of the Year Award (2018), and the Robert Dawes Evans Senior Research Mentor Award from Boston University.
Original Post
View all posts

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- J Healthc Eng
- v.2023; 2023
Lung Diseases Detection Using Various Deep Learning Algorithms
M. jasmine pemeena priyadarsini.
1 School of Electronics Engineering, Vellore Institute of Technology, Vellore 632014, India
Ketan kotecha
2 Symbiosis Centre for Applied Artificial Intelligence, Symbiosis International (Deemed University), Pune, India
3 School of Mathematical Sciences, Sunway University, Subang Jaya, Malaysia
G. K. Rajini
4 School of Electrical Engineering, Vellore Institute of Technology, Vellore 632014, India
K. Hariharan
K. utkarsh raj, k. bhargav ram, v. indragandhi, v. subramaniyaswamy.
5 School of Computing, SASTRA Deemed University, Thanjavur, India
Sharnil Pandya
6 Computer Science and Media Technology Department, Faculty of Technology, Linnaeus University, P G Vejdes väg 351 95, Växjö, Sweden
Associated Data
The data used to support the findings of this study are available from the corresponding author upon request.
The primary objective of this proposed framework work is to detect and classify various lung diseases such as pneumonia, tuberculosis, and lung cancer from standard X-ray images and Computerized Tomography (CT) scan images with the help of volume datasets. We implemented three deep learning models namely Sequential, Functional & Transfer models and trained them on open-source training datasets. To augment the patient's treatment, deep learning techniques are promising and successful domains that extend the machine learning domain where CNNs are trained to extract features and offers great potential from datasets of images in biomedical application. Our primary aim is to validate our models as a new direction to address the problem on the datasets and then to compare their performance with other existing models. Our models were able to reach higher levels of accuracy for possible solutions and provide effectiveness to humankind for faster detection of diseases and serve as best performing models. The conventional networks have poor performance for tilted, rotated, and other abnormal orientation and have poor learning framework. The results demonstrated that the proposed framework with a sequential model outperforms other existing methods in terms of an F1 score of 98.55%, accuracy of 98.43%, recall of 96.33% for pneumonia and for tuberculosis F1 score of 97.99%, accuracy of 99.4%, and recall of 98.88%. In addition, the functional model for cancer outperformed with an accuracy of 99.9% and specificity of 99.89% and paves way to less number of trained parameters, leading to less computational overhead and less expensive than existing pretrained models. In our work, we implemented a state-of-the art CNN with various models to classify lung diseases accurately.
1. Introduction
Lungs play a vital role in the human system, which performs expansion and relaxation to bring in oxygen and take out carbon dioxide. Lung diseases are respiratory diseases that affect the various organs and tissues associated with breathing, leading to airway diseases, lung tissue diseases, and lung circulation diseases. Some of the respiratory diseases like common cold and influenza cause mild discomfort and hindrance while others like pneumonia, tuberculosis and lung cancer are life-threatening and cause severe acute respiratory problems [ 1 ].
According to a research study done by the Forum of International Respiratory Societies called “The Global Impact of Respiratory Disease,” 10.4 million people suffered mild or severe symptoms of tuberculosis, and 1.4 million of those affected died as per the survey reported [ 2 ]. Lung cancer kills an astounding number of people every year. More than 1.6 million people were reported to have died in the year the survey was carried out. Pneumonia is one of the top respiratory diseases and 1.23 million children under the age of 5 died due to pneumonia according to the Johns Hopkins Bloomberg School of Public Health report titled “Pneumonia and Diarrhea Progress Report 2020” [ 3 ]. Detection of the abovementioned diseases at the early stages of infection can drastically increase the chances of survival and can prevent human casualities. Chest X-ray images and CT scans are common examinations that determine the presence of these diseases [ 4 ]. The presence of trained professionals is required to examine the scanned images and determine the infections. According to the Union Health Ministry data statistics there exists a shortfall of 76.1 percent of physicians at the Community Health Centres (CHCs) in rural areas. To overcome this, deep learning techniques are implemented, which pave the way for a new strategy.
Deep learning is a branch of machine learning that provides state-of-the-art accuracy and is a subset of the artificial intelligence with representation learning. This tool has drawn attention in recent times due to their ability to read image data, process them, and provide results based on the previously trained data [ 5 ]. Deep learning models can learn features and patterns from dataset images and use the learned features to classify new test images that have not been previously visualized by the model.
Numerous works have already been conducted by researchers around the world and have led to promising results. These works can help support existing methods or open pathways to new ones that could not have been possible. These advancements can help in quick and accurate detection as well as classification of diseases and provide quick support to obtain impressive results to eliminate deadly infectious diseases.
The rest of the manuscript is structured as follows: In Section 2 , we introduce the basic foundation of the convolution neural networks. Section 3 describes the architecture of the proposed model. Section 4 discusses the implementation of the proposed CNN technique and the experimental results. Finally, we conclude our work with a summary and future directions in Section 5 .
2. Related Work
One of the best techniques currently used in medical image analysis are CNNs, which have a remarkable efficiency in classifying the images. Some of the contemporary CNN models are Pre-Trained, Functional, and Sequential, which are reviewed in the forthcoming sections.
Liu et al. proposed three different types for the applications of CNN-trained models in tuberculosis detection. In all these three methods, features are extracted by the CNN architectures and are trained by the support vector machine (SVM), and in the second proposal, features are extracted from coreference resolution (CR) and are trained in the SVM classifier. In the third proposal, these two proposals are combined together to create an ensemble of the classifiers. The Montgomery dataset has a total of 138 X-ray images and the Shenzhen dataset has a total of 662 X-ray images. These trained models help reduce the processing time but provide low accuracy, which is not conducive and cannot be implemented in medical diagnosis.
Amit Kumar Jaiswal, Prayag Tiwari, Sachin Kumar, and Deepak Gupta proposed a method called mask RCNN. It is a deep neural network model that can extract two types of features: global and local. Pixel-wise division is carried out and this method is expected to have a better performance evaluated on the radiograph dataset. This technique highlights the infected regions and provides a heat map for better understanding for people looking at the results. But they have ensembled ResNet50 and ResNet101 (Mask RCNN models) but achieved less biased results than expected and require more GPU processing power to train.
Elshennawy and Ibrahim, presented on four different models. Among these four models, CNN and LSTM-CNN started from the beginning and the other two are pretrained models and the specific models used are ResNet152v2 and MobileNetV2. They formulated to create from the ground, a deep learning neural network model, which could diagnose pneumonia symptoms using chest X-ray images, which has pneumonia [ 6 ]. Some of the disadvantages are that it has a humongous architecture with hundreds of millions of trainable parameter weights [ 7 , 8 ]. This type of model requires high computing and processing power.
Various deep learning techniques, Naik and Edla [ 9 ] developed a lung nodule classification and identification model for computed tomography (CT) images. The CT scans required a computer-aided detection system for categorizing the lung nodule into benign and malignant types, along with the highest level of accuracy to protect from a delay in diagnosis. The deep learning approaches used to categorize the lung nodule have positive outcomes compared to other methods. When the mutations were implemented in the deep learning architecture, the accuracy of the classification system increased rapidly. The deep learning method was used to specify the new impacts in nodule classification and also recognized the preliminary stage of a malignant lesion [ 10 ].
3. Proposed Methodology
This section discusses the datasets used, the preprocessing, the data augmentation methods, and the various algorithms used. The workflow of the proposed technique is presented in a flowchart form in Figure 1 .

Workflow of the classification model.
3.1. Datasets
All the datasets used in this work are from opensource datasets published on the website “Kaggle.”
The pneumonia dataset published by Paul Mooney contains 5,856 frontal chest X-ray images, 1,583 images of the dataset are of people with no abnormalities in their lungs, and 4,273 images predict some abnormalities and symptoms of pneumonia.
The tuberculosis dataset published by Scott Mader has 662 frontal X-rays. These images were collected by physicians in the Guangdong Hospital, Shenzhen, China. Hence, this dataset is commonly known as the Shenzhen dataset. It contains 326 images, which contains lung images of healthy persons and in turn contains 336 images that are infected by tuberculosis.
The cancer dataset published by Mohamed Hany has 907 lung CT-scan images, 215 images of the dataset are of people with no signs of cancer, and 692 images of the dataset are of people with cancer. The dataset contains 3 types of cancer images: adenocarcinoma, large cell carcinoma, and squamous cell carcinoma. Figure 2 shows few sample images from the CT-scan dataset.

Chest-CT scan images (source: kaggle).
3.1.1. Preprocessing and Data Augmentation
The images present in the datasets are of different resolutions. However, the CNN models require images to be of one specified size. Hence, all the images in the dataset were resized to 224 × 224. Lowering the input image size helps process a faster execution of images and thus, makes the model faster for the specific associated task.
Data augmentation is a common support method used to significantly increase the training data volume by introducing slight variations of an image in each training epoch. The variations used in this work are horizontal flip, zoom, shear, rotation, and rescale. This technique is essential to get high levels of accuracy as the CNN model is able to train on more data than originally present in the dataset. Figure 3 shows the variations that can be created from one sample image.

Variations of a chest X-ray image.
3.2. Deep Learning Algorithms
In recent times, a dataset of medical images has been available in the Kaggle repository. In this paper, this dataset has been implemented using the novel models of CNN, namely, sequential and functional models, combining CNN and data augmentation. Three different model algorithms were deployed in this proposed work. These are explained in detail in the following subsections.
3.2.1. Sequential Model
The sequential model is a model in which layers are stacked to form a sequential order. The input is passed through all the layers in the order in which the layers are stacked. Features are learnt at each and every layer and more deeper into the layer, the model is capable of distinguishing the infected areas and noninfected areas from the chest X-rays [ 11 ].
The proposed sequential model has five convolutional layers with the number of filters increasing as it proceeds deeper into the network [ 12 ]. The alpha parameter was set to 0.66. Leaky ReLU allows a small gradient to pass through, while ReLU completely removes any gradient when the unit is not active. In addition, max pooling was carried out after each activation. Adam optimizer and learning rate of 0.0001 was employed. The block diagram of the sequential model is presented in Figure 4 .

Block diagram of sequential model.
3.2.2. Functional Model
The functional model has more flexibility than the other algorithms. It can form connections between any two layers contrary to the others and progress in a linear fashion. This allows us to create more complicated and sophisticated networks [ 13 ]. The input goes through the first layer and then proceeds along the designed architecture. This method also trains from the beginning, contrary to the pretrained model.
The proposed functional model has two convolution layers of 7 × 7 window and another with 1 × 1 on top of 3 × 3 window as presented in Figure 5 . The input is passed through both convolution layers separately and then the output from both layers is appended and then passed to five 3 × 3 convolution layers. The Adam optimizer with learning rate = 0.0001 was employed.

Block diagram of functional model.
3.2.3. Pretrained Model
This is the easiest and most commonly used model for image classification. Instead of training a model from the beginning, this technique uses already trained weights on a large dataset of images to classify the required images [ 14 , 15 ]. This technique is also called transfer learning as previously learned weights are transferred and used for classification. Generally, this model takes less time to train and produces better results and accuracy.
The pretrained model used here is VGG-16, a convolutional neural network (CNN), famous for high accuracy and achieved the top 5 accuracies in the ImageNet competition with an accuracy of 97.7%.
4. Results and Discussion
The various models were trained, their accuracies and losses were plotted, and the test accuracy was obtained and compared with other research works for lung disease detection with CNN [ 16 , 17 ]. The performance metrics involved in this proposed work are accuracy, precision, recall, and F1 score.
- (i) Accuracy represents the number of correctly classified data instances over the total number of data instances. A c c u r a c y = T P + T N T P + T N + F P + F N , (1) where, true positive is abbreviated as TP, true negative as TN, false positive as FP, and false negative as FN.
- (ii) Precision should ideally be 1 (high) for a good classifier. Precision becomes 1 only when the numerator and denominator are equal, i.e, TP = TP + FP, this also means FP is zero. As FP increases, the value of the denominator becomes greater than the numerator and the precision value decreases. p r e c i s i o n = T P T P + F P . (2)
- (iii) Recall is also known as sensitivity or true positive rate and is defined as follows: R e c a l l = T P T P + F N . (3)
- (iv) F1-score is a metric that takes into account both precision and recall and is defined as follows: F 1 s c o r e = 2 ∗ p r e c i s i o n ∗ R e c a l l p r e c i s i o n + R e c a l l . (4)
4.1. Sequential Model for Pneumonia
In medical diagnostics, it is common to analyze the classifier performance using sensitivity (true positive rate) and specificity (true negative rate) instead of accuracy [ 6 ]. To assess the overall classification F1 score is computed [ 7 , 18 ]. From the dataset of 5,856 chest X-ray images, 2,000 images were used for training of which 1,000 images were of normal chest X-rays and the other 1,000 images were of pneumonia-infected chest X-rays.
The model was trained for 50 epochs. Figure 6 shows the increase in accuracy as the model trains with trained set images and Figure 7 shows that the loss encountered with this model is less. The accuracy starts from 75% and gradually increases to 90% with 10 epochs.

Model accuracy vs. epochs for pneumonia (sequential).

Model loss vs. epochs for pneumonia (sequential).
After training, the model was used to predict the labels of test images that were not known by the model during training. The test image set had 583 images of normal chest X-rays and 3,273 images of pneumonia-infected chest X-rays. Table 1 provides accuracy of our model with the existing works related to pneumonia and found that our model outperforms other existing works. The model predicted the labels accurately for 533 images from 583 normal CXR images and 3,070 images from 3,273 pneumonia-infected CXR images.
Comparison of our model with existing works related to pneumonia.
4.2. Sequential Model for Tuberculosis
The tuberculosis dataset has a grand total of 662 chest X-ray images. Among 662 images, 285 images of normal chest X-rays and 292 images of tuberculosis-infected chest X-rays were used for training. As depicted in Figure 8 , the tuberculosis model started with a very low accuracy of 50%. After training for around 100 epochs, the model accuracy value of 97% was obtained.

Model accuracy vs. epochs for tuberculosis.
Numerous works have already been carried out by researchers around the world and have led to promising results. These works can help support the existing methods or open pathways to new methods, which could not have been possible before [ 8 , 24 ]. These advancements can help in faster and accurate detection, as well as classification of diseases and provide support to obtain impressive results to eliminate deadly infectious diseases.
The model was used to predict the labels for test images. The test image set had a total of 85 images of which 41 were of normal and 44 were of tuberculosis-infected. The model predicted 37 images of normal and 39 images of tuberculosis-infected accurately as presented in Figure 9 . Table 2 provides an accuracy of our model with existing works related to tuberculosis and finds to be superior when compared to other existing works.

Model loss vs. epochs for tuberculosis.
Accuracy of our model with existing works related to tuberculosis.
4.3. Functional Model for Cancer
The dataset has a total of 907 lung CT-scan images, 215 images of people with no signs of cancer, and 692 images of people infected with cancer were used for training the model [ 30 , 31 ]. The model was trained for 100 epochs. As seen in Figure 10 , the model started with an accuracy of 70% and increased to 90% in about 10 epochs.

Model accuracy vs. epochs for cancer.
The model was presented to predict for the test images. The test dataset had a total of 278 images, of which 224 were cancer infected and 54 were normal. The model accurately predicted 54 images of normal and 204 images of cancer infected, and the loss is shown in Figure 11 .

Model loss vs. epochs for cancer.
Table 3 depicts the accuracy of our model with existing works related to cancer and finds to be extraordinary when compared to other existing works.
Accuracy of our model with existing works related to cancer.
4.4. Functional Model for Pneumonia
The dataset used for the functional model is the one that was utilized in sequential model. The model accuracy starts from around 81% and rapidly increases to 90% in less than 5 epochs.
4.5. Pretrained Model for Pneumonia
Figure 12 shows the model accuracy gradual improvement for the pneumonia disease with the functional model. The same dataset was used for this model, i.e., from Paul Mooney with 5,856 images of which 1,000 are normal X-rays and other 1,000 are infected chest X-rays. As the model has already been trained before, the starting accuracy is very good. There is a minor improvement after training for 15 epochs as is evident in Figure 13 .

Model accuracy vs. epochs for pneumonia (functional).

Model loss vs. epochs for pneumonia (functional).
Figure 14 shows that the initial model loss is low as compared to the other models, hence, there is no continuous progress like that in the sequential and functional models.

Model accuracy vs. epochs for pneumonia (pretrained).
Figure 15 shows that the pretrained models are easy to train and that the loss gradually decreases as they have previously been trained on various datasets.

Model loss vs. epochs for pneumonia (pretrained).
5. Conclusion and Future Work
We have proposed three different architecture models of CNNs, which were used to train on various lung diseases that are available in the open-source dataset. The trained models were used to predict the labels of some test images that were not visualized by the models. The results of the proposed models performed better than other related works. The results obtained through this framework with a sequential model outperform other existing methods in terms of F1 score, accuracy and recall for pneumonia and for tuberculosis. In addition, the functional model for cancer outperformed with accuracy and specificity, and it requires less computation cost and time. In future, varying the optimizers, learning rate, and introduction of more data augmentation could potentially lead to further improvements in the classification accuracy of the proposed CNN models. Early stopping techniques will likely provide further insights into diagnosing lung diseases that can be passed down to avoid overfitting.
Data Availability
Conflicts of interest.
The authors declare that there are no conflicts of interest regarding the publication of this paper.

Black Lung cases rise, as federal benefits stagnate
Current monthly benefits for a miner and one dependent in 2024 are around $1,100, more than $3,000 lower than the average cost of living for a two-person household.
Quenton King, federal legislative specialist for Appalachian Voices, said lagging benefits are especially troubling when miners are increasingly developing black lung at younger ages, largely due to exposure to toxic silica dust.
"Younger miners are getting diagnosed with stage-three black lung, and they're having to quit mining in their 30s or 40s," King observed. "They're losing possibly 20 years, 30 years of work history, and they're unable to draw down that retirement fund."
Around 16% of the nation's coal workers are living with black lung, and after decades of improvement, the number of cases is on the rise again, according to the American Lung Association.
One National Institute for Occupational Safety and Health study found modern coal miners, particularly those in Central Appalachia, are more likely than their predecessors to die from coal worker's pneumoconiosis, chronic obstructive pulmonary disease and lung cancer.
King pointed out although the coal industry in on the decline, thousands of coal miners and their families living in Appalachian communities are affected daily by the disease.
"Something I hear from people in the Black Lung Association, one of the heartbreaking things for me is that they're not able to play with their grandchildren, because they are on oxygen tanks," King noted.
Appalachian advocacy groups sent a letter to Congress asking for budget legislation prioritizing investments in curbing black lung and supporting miners already living with the disease. Proposed federal legislation, known as the Black Lung Benefits Improvement Act , would tie benefit levels to cost-of-living adjustments, rather than the federal pay scale.
.")
Researchers identify protein sensor that plays a role in lung fibrosis
Researchers at Weill Cornell Medicine have discovered a protein called SEL1L that plays a critical role in clearing collagen from tissue, and which may be a therapeutic target to help prevent fibrosis, scar tissue that interferes with organ function. The paper, published on Feb. 20 in Nature Communications, provides clues that could lead to drug development for diseases like lung fibrosis which have no therapeutic options currently.
Corresponding author, Dr. Michael J. Podolsky, assistant professor of medicine at Weill Cornell Medicine, has led a team that searched the human genome for genes involved in the process that triggers specialized cells to engulf and digest excess collagen from tissue. Cells called fibroblasts and macrophages pick up collagen fragments for degradation in lysosomes, the trash compactors of cells.
Normal lungs continuously synthesize collagen and degrade excess collagen, keeping the two processes precisely balanced to maintain healthy tissue architecture. Even when lungs are injured and the body responds by increasing the rate of collagen production, simultaneously collagen degradation is increased to prevent the formation of permanent scar tissue. However, when the two processes are uncoupled, the result is disease. In pulmonary fibrosis, for instance, collagen degradation does not keep pace with collagen production, resulting in an excess accumulation.
The researchers discovered a mechanism that cells use to detect collagen production internally and regulate clearance of excess collagen in tissues. The protein SEL1L acts as a sensor that responds to collagen production by triggering another protein called MRC2 which is involved in the uptake and disposal of collagen.
This study suggests that a defective collagen clearing pathway based on MRC2 is a key part of the imbalance in fibrotic disease. The data show when SEL1L is overproduced in cells, it leads to increased MRC2 production and thereby prevents the accumulation of collagen. This pathway could eventually be therapeutically targeted to drive increased clearance of collagen to improve fibrosis when it is impaired. Next, Dr. Podolsky, who is also an attending physician at NewYork Presbyterian/Weill Cornell Medical Center, plans to investigate how SEL1L is impaired in fibrotic human lungs. The lab is also exploring the molecular consequences of when MRC2 is inadequately triggered in pulmonary fibrosis.
This research was supported in part by the National Institutes of Health grant K08 HL145015 and a Grant-in-aid from The Stony Wold-Herbert Fund.
- Cystic Fibrosis
- Hypertension
- Lung Disease
- Medical Topics
- Diseases and Conditions
- Personalized Medicine
- Cystic fibrosis
- Drug discovery
- Gene therapy
- Adipose tissue
Story Source:
Materials provided by Weill Cornell Medicine . Note: Content may be edited for style and length.
Journal Reference :
- Michael J. Podolsky, Benjamin Kheyfets, Monika Pandey, Afaq H. Beigh, Christopher D. Yang, Carlos O. Lizama, Ritwik Datta, Liangguang L. Lin, Zhihong Wang, Paul J. Wolters, Michael T. McManus, Ling Qi, Kamran Atabai. Genome-wide screens identify SEL1L as an intracellular rheostat controlling collagen turnover . Nature Communications , 2024; 15 (1) DOI: 10.1038/s41467-024-45817-8
Cite This Page :
Explore More
- Illuminating Oxygen's Journey in the Brain
- DNA Study IDs Descendants of George Washington
- Heart Disease Risk: More Than One Drink a Day
- Unlocking Supernova Stardust Secrets
- Why Do Some Memories Become Longterm?
- Cell Division Quality Control 'Stopwatch'
- What Controls Sun's Differential Rotation?
- Robot, Can You Say 'Cheese'?
- Researchers Turn Back the Clock On Cancer Cells
- Making Long-Term Memories: Nerve-Cell Damage
Trending Topics
Strange & offbeat.
- Skip to main content
- Keyboard shortcuts for audio player
Amid a black lung surge, Kentucky has made it harder for coal miners to get benefits
Justin Hicks
Kentucky has one black lung doctor left after the state legislature restricted who can review workers' compensation claims for the disease. This came amid a surge in black lung cases in Appalachia.

Shots - Health News
As coal miners suffer and die from severe black lung, a proposed fix may fall short.
AILSA CHANG, HOST:
There is only one doctor left in Kentucky who can officially diagnose miners with black lung disease so that they can get worker's compensation benefits. Kentucky Public Radio's Justin Hicks reports that that is partly due to a restrictive law passed by the state legislature six years ago. Some lawmakers are trying to change that.
JUSTIN HICKS, BYLINE: Brandon Crum's radiology clinic is in a former Walmart in Pikeville, Ky.
(SOUNDBITE OF PHONE RINGING)
HICKS: Each day, former coal miners come in gasping for air. He ushers them into an X-ray room to take a look.
BRANDON CRUM: That one X-ray that it takes maybe three minutes to do sums up an entire 20- or 30-year history of working in the mines.
HICKS: Many of Crum's patients are diagnosed with black lung. It's an incurable and fatal disease that's been directly linked to coal mining. Research has proven there's a surge of black lung now in Appalachia. Despite his detailed X-rays and patient histories, the state won't refer miners to Crum in order to determine if they should get worker's compensation benefits in Kentucky.
CRUM: I know of nowhere in the United States of America or the world except Kentucky where radiologists cannot read chest X-rays to diagnose a disease.
HICKS: It wasn't always this way. Kentucky used to let radiologists who specialized in coal dust do this work. But in 2018, Kentucky lawmakers changed things so that only pulmonologists can make the official black lung diagnosis. Crum says lawmakers did it to cover up a rise in the deadly disease among coal miners.
CRUM: Because I found too much black lung and complicated black lung. It's the truth.
HICKS: At the time, the coal industry testified that the law was to make diagnosis less subjective. Tyler White, who was president of the Kentucky Coal Association then, said the bill would combat their rising insurance premiums.
TYLER WHITE: These staggering increases deal a significant blow to employers and the overall cost of workers' compensation in Kentucky and now places the Kentucky coal industry at a material disadvantage to neighboring states.
HICKS: Just before the law went into effect, there were 10 doctors allowed to judge Kentucky black lung claims. Then, once fewer doctors were eligible, the rate of miners who were approved for benefits dropped drastically. Today, there's only one doctor who is screening black lung for workers' comp in the state. His name is Dr. Srinivas Ammisetty. He declined to be interviewed.
DOUG HOLLIDAY: He's a very nice person, an honest doctor, a fair doctor, but he's fallible just like anybody else.
HICKS: That's Doug Holliday. As a worker's comp attorney in Hazard, he's very familiar with Dr. Ammisetty, and he says the doctor has become the decisive voice for all of these cases.
HOLLIDAY: If a miner does not agree with the opinion that he has, he ought to have an opportunity to present evidence on the same footing that Dr. Ammisetty stands on.
HICKS: There's efforts to change this, though. Democratic State Representative Ashley Tackett Laferty says it's one of the reasons she ran for office.
ASHLEY TACKETT LAFERTY: There were quite a few bills that were harmful to our coal miners. So definitely, it was certainly a big motivation.
HICKS: Tackett Laferty is carrying a bill this year that would allow radiologists to give their medical opinions to the workers' comp board again, but even she wasn't aware there was only one doctor still participating.
LAFERTY: Well, I am glad to hear that this doctor is located in the vicinity of eastern Kentucky, but, yeah, that concerns me.
HICKS: The bill has been proposed before. But just like those other attempts, this year's version hasn't moved at all.
LAFERTY: We've really been working to try to bring it to the forefront, but, just, it seems like - that it's not working.
HICKS: Until then, coal miners seeking compensation from the mines they believe diseased them will continue to go to Dr. Ammisetty. Ammisetty says he plans to continue diagnosing black lung claims, although he closed his office in Pikeville at the start of the year.
For NPR News, I'm Justin Hicks in Pikeville, Ky.
(SOUNDBITE OF RAPSODY AND HIT-BOY SONG, "ASTEROIDS")
Copyright © 2024 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by an NPR contractor. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
IMAGES
COMMENTS
Abstract. Coal workers' pneumoconiosis (CWP), commonly known as black lung, is caused by the inhalation of respirable coal mine dust and is a disabling and potentially fatal lung disease with no cure. Historically, CWP has taken a tremendous human and financial toll in the US coal mining industry. Recent health surveillance data indicates ...
Submit your paper; Open access ... however, there is a tendency to be complacent about health risks, leading to an assumption that black lung disease is no longer a threat. This is simply not true. Deborah Yates (St Vincent's Hospital, NSW, Australia) has accumulated many years of experience in occupational lung disease research, training, and ...
Abstract. Coal workers' pneumoconiosis (CWP), commonly known as black lung, is caused by the inhalation of respirable coal mine dust and is a disabling and potentially fatal lung disease with no cure. Historically, CWP has taken a tremendous human and financial toll in the US coal mining industry. Recent health surveillance data indicates that ...
Progressive massive fibrosis (PMF) is the most severe and disabling form of coal workers' pneumoconiosis. 1 Between January 2013 and February 2017, 416 cases were identified in miners in 3 federally funded Black Lung Clinics in Virginia (Stone Mountain Health Services [SMHS]). To our knowledge, this is the largest reported cluster of PMF in the scientific literature. 1 In 2019, the Health ...
Black lung attorneys interviewed in this research discussed the importance of broadening diagnoses of the disease to capture the full range of environmental health impacts on miners. An attorney described the basic clinical diagnosis of black lung, describing CWP and PMF, and then described the broader parameters of a 'legal definition' of ...
In particular, the past decade has seen four major changes to the federal law concerning black lung. First, in 2014, the U.S. Department of Labor ("DOL") made the first changes since 1972 to the regulations limiting the dust that miners breathe while working underground. The Dust Rule reduces the permissible dust level by 25%, closes ...
Subsequent investigations have reported that black lung cases have tripled and that tenured miners in central Appalachia, the epicenter of the disease, have experienced a tenfold increase in ...
Black lung disease data based on secondary data from the National Health Commission of China, 2019. In 1990-2019, there were 4974 (4.97%) cases of black lung disease. CWP was mainly caused by male groups and more elderly miners (OR/95% CI = N/A) The prevalence of black lung disease during 1990-2019 in China is 4.97%.
Abstract. The black lung movement that erupted in West Virginia in 1968 was not simply a struggle for recognition of an occupational disease; it grew into a bitter controversy over who would control the definition of that disease. This article examines the historical background and medical politics of that controversy, arguing that black lung ...
The first new pathology standards for black lung disease in more than 50 years were published based on research from the UIC School of Public Health's Mining Education and Research Center. ... "It's a smoking gun that something has to change to prevent this disease." In a second paper, an international panel of pathologists looked at 85 ...
Coal workers' pneumoconiosis, also known as "black lung disease," is an occupational lung disease caused by overexposure to respirable coal mine dust. Inhaled dust leads to inflammation and fibrosis in the lungs, and coal workers' pneumoconiosis can be a debilitating disease. ... Previous research found that 25 of 37 (68%) ...
The study, published in the September 2018 American Journal of Public Health, highlights that black lung is not a disease of antiquity but results from injurious exposures to coal miners today. Although PMF was rarely seen in miners who participated in the CWHSP throughout the 1990s, in 2018, according to a JAMA research letter, PMF was ...
and black lung disease—and a statistical analysis of publicly available data from various time periods spanning 1970-2021 to identify black lung incidence, determine whether ... research development process includes extensive technical review at the design, data collection and analysis stage, including: external contractor review and OMB ...
Chronic obstructive pulmonary disease (COPD) is a progressive, debilitating respiratory condition and currently the third leading cause of death in the United States ().Though over 11 million people have been diagnosed with COPD, many more have undiagnosed disease ().This number is projected to increase further as America's population ages.
The remainder of this paper synthesizes the available literature on black lung disease to answer the research question "What is the current state of knowledge on black lung disease, particularly as it relates to coal mining, residential coal use, Appalachian populations, and Navajo Nation residents?" Findings are organized as follows:
Lung function impairment and rapidly progressing lung disease have been increasingly described in coal miners with relatively short mining tenures due to intense dust exposures. Coal mining-related exposures including silica dust and diesel exhaust are likely to account for recent analyses showing an association between coal mining and lung ...
About the Study. In 2022, the Chief Evaluation Office (CEO) partnered with the Mine Safety and Health Administration (MSHA) and commissioned contractor Summit Consulting, LLC (Summit) to conduct the Black Lung Incidence Study under the Administrative Data Research and Analysis portfolio of studies. This study uses secondary data to examine the rate of black lung disease across the United ...
those with black lung disease and silicosis particularly hard. Unfortunately, the risk of developing CWP from a coal mining career is high, and in some areas the risk has gotten higher.
Two recent papers from the center expand upon this link, with both comparing the lungs of miners from the mid-20th century with those from more recent cases of black lung disease. The studies are the first update on the pathology of black lung disease since 1971, highlighting features in lung tissue that are unique to this newer version and ...
Black Lung Disease (Coal Workers' Pneumoconiosis) Black lung disease is inflammation and scarring common among people who work in coal mines. Some people may not have symptoms. Others may have difficulty breathing, cough up black mucus and experience chest tightness. Medications can help ease symptoms, but there's no cure.
Coal workers' pneumoconiosis (CWP), commonly known as black lung, is caused by the inhalation of respirable coal mine dust and is a disabling and potentially fatal lung disease with no cure. Historically, CWP has taken a tremendous human and financial toll in the US coal mining industry. Recent health surveillance data indicates that CWP continues to occur at elevated levels. Respirable coal ...
The paper, published on Feb. 20 in Nature Communications, provides clues that could lead to drug development for diseases like lung fibrosis which have no therapeutic options currently.
A team of researchers led by Darrell N. Kotton, MD, the David C. Seldin Professor of Medicine, has been awarded a five-year, $14 million grant from the NIH's National Heart, Lung, and Blood Institute (NHLBI) for his research, "Developing Pluripotent Stem Cells to Model and Treat Lung Disease." Lung diseases, such as those caused by gene ...
2.2 Literature review on black lung disease in the Navajo Nation . Summit conducted a literature review to assess the current state of research on black lung disease. 5. One area of focus within that literature review was black lung incidence due to coal mining or residential coal use within the Navajo Nation.
According to a research study done by the Forum of International Respiratory Societies called "The Global Impact of Respiratory Disease," 10.4 million people suffered mild or severe symptoms of tuberculosis, and 1.4 million of those affected died as per the survey reported . Lung cancer kills an astounding number of people every year.
The benefit payments miners sick with black lung disease receive are not keeping pace with the cost of living, a new analysis showed. Current monthly benefits for a miner and one dependent in 2024 ...
The paper, published on Feb. 20 in Nature Communications, provides clues that could lead to drug development for diseases like lung fibrosis which have no therapeutic options currently.
Kentucky has one black lung doctor left after the state legislature restricted who can review workers' compensation claims for the disease. This came amid a surge in black lung cases in Appalachia.
Lung cancer is one of the most prevalent cancers in the world and is responsible for most cancer-related fatalities. The present methods for identifying lung cancer, such as CT scans and biopsies, have drawbacks, such as being expensive, intrusive, and exposing patients to radiation. Convolutional neural networks (CNN), deep learning, and other machine learning approaches have recently ...