Obstetrics and gynaecology
Showing results 1 - 10 of 100
Sorted by most recent
2 April 2024
27 March 2024
25 March 2024
22 March 2024
21 March 2024
19 March 2024
- Remote Access
- Save figures into PowerPoint
- Download tables as PDFs


Introduction
- Download Chapter PDF
Disclaimer: These citations have been automatically generated based on the information we have and it may not be 100% accurate. Please consult the latest official manual style if you have any questions regarding the format accuracy.
Download citation file:
- Search Book
Jump to a Section
- Full Chapter
- Supplementary Content
Pop-up div Successfully Displayed
This div only appears when the trigger link is hovered over. Otherwise it is hidden from view.
Please Wait
- Search Menu
- Browse content in Arts and Humanities
- Browse content in Archaeology
- Anglo-Saxon and Medieval Archaeology
- Archaeological Methodology and Techniques
- Archaeology by Region
- Archaeology of Religion
- Archaeology of Trade and Exchange
- Biblical Archaeology
- Contemporary and Public Archaeology
- Environmental Archaeology
- Historical Archaeology
- History and Theory of Archaeology
- Industrial Archaeology
- Landscape Archaeology
- Mortuary Archaeology
- Prehistoric Archaeology
- Underwater Archaeology
- Urban Archaeology
- Zooarchaeology
- Browse content in Architecture
- Architectural Structure and Design
- History of Architecture
- Residential and Domestic Buildings
- Theory of Architecture
- Browse content in Art
- Art Subjects and Themes
- History of Art
- Industrial and Commercial Art
- Theory of Art
- Biographical Studies
- Byzantine Studies
- Browse content in Classical Studies
- Classical History
- Classical Philosophy
- Classical Mythology
- Classical Literature
- Classical Reception
- Classical Art and Architecture
- Classical Oratory and Rhetoric
- Greek and Roman Epigraphy
- Greek and Roman Law
- Greek and Roman Archaeology
- Greek and Roman Papyrology
- Late Antiquity
- Religion in the Ancient World
- Digital Humanities
- Browse content in History
- Colonialism and Imperialism
- Diplomatic History
- Environmental History
- Genealogy, Heraldry, Names, and Honours
- Genocide and Ethnic Cleansing
- Historical Geography
- History by Period
- History of Agriculture
- History of Education
- History of Emotions
- History of Gender and Sexuality
- Industrial History
- Intellectual History
- International History
- Labour History
- Legal and Constitutional History
- Local and Family History
- Maritime History
- Military History
- National Liberation and Post-Colonialism
- Oral History
- Political History
- Public History
- Regional and National History
- Revolutions and Rebellions
- Slavery and Abolition of Slavery
- Social and Cultural History
- Theory, Methods, and Historiography
- Urban History
- World History
- Browse content in Language Teaching and Learning
- Language Learning (Specific Skills)
- Language Teaching Theory and Methods
- Browse content in Linguistics
- Applied Linguistics
- Cognitive Linguistics
- Computational Linguistics
- Forensic Linguistics
- Grammar, Syntax and Morphology
- Historical and Diachronic Linguistics
- History of English
- Language Acquisition
- Language Variation
- Language Families
- Language Evolution
- Language Reference
- Lexicography
- Linguistic Theories
- Linguistic Typology
- Linguistic Anthropology
- Phonetics and Phonology
- Psycholinguistics
- Sociolinguistics
- Translation and Interpretation
- Writing Systems
- Browse content in Literature
- Bibliography
- Children's Literature Studies
- Literary Studies (Asian)
- Literary Studies (European)
- Literary Studies (Eco-criticism)
- Literary Studies (Modernism)
- Literary Studies (Romanticism)
- Literary Studies (American)
- Literary Studies - World
- Literary Studies (1500 to 1800)
- Literary Studies (19th Century)
- Literary Studies (20th Century onwards)
- Literary Studies (African American Literature)
- Literary Studies (British and Irish)
- Literary Studies (Early and Medieval)
- Literary Studies (Fiction, Novelists, and Prose Writers)
- Literary Studies (Gender Studies)
- Literary Studies (Graphic Novels)
- Literary Studies (History of the Book)
- Literary Studies (Plays and Playwrights)
- Literary Studies (Poetry and Poets)
- Literary Studies (Postcolonial Literature)
- Literary Studies (Queer Studies)
- Literary Studies (Science Fiction)
- Literary Studies (Travel Literature)
- Literary Studies (War Literature)
- Literary Studies (Women's Writing)
- Literary Theory and Cultural Studies
- Mythology and Folklore
- Shakespeare Studies and Criticism
- Browse content in Media Studies
- Browse content in Music
- Applied Music
- Dance and Music
- Ethics in Music
- Ethnomusicology
- Gender and Sexuality in Music
- Medicine and Music
- Music Cultures
- Music and Religion
- Music and Culture
- Music and Media
- Music Education and Pedagogy
- Music Theory and Analysis
- Musical Scores, Lyrics, and Libretti
- Musical Structures, Styles, and Techniques
- Musicology and Music History
- Performance Practice and Studies
- Race and Ethnicity in Music
- Sound Studies
- Browse content in Performing Arts
- Browse content in Philosophy
- Aesthetics and Philosophy of Art
- Epistemology
- Feminist Philosophy
- History of Western Philosophy
- Metaphysics
- Moral Philosophy
- Non-Western Philosophy
- Philosophy of Science
- Philosophy of Action
- Philosophy of Law
- Philosophy of Religion
- Philosophy of Language
- Philosophy of Mind
- Philosophy of Perception
- Philosophy of Mathematics and Logic
- Practical Ethics
- Social and Political Philosophy
- Browse content in Religion
- Biblical Studies
- Christianity
- East Asian Religions
- History of Religion
- Judaism and Jewish Studies
- Qumran Studies
- Religion and Education
- Religion and Health
- Religion and Politics
- Religion and Science
- Religion and Law
- Religion and Art, Literature, and Music
- Religious Studies
- Browse content in Society and Culture
- Cookery, Food, and Drink
- Cultural Studies
- Customs and Traditions
- Ethical Issues and Debates
- Hobbies, Games, Arts and Crafts
- Lifestyle, Home, and Garden
- Natural world, Country Life, and Pets
- Popular Beliefs and Controversial Knowledge
- Sports and Outdoor Recreation
- Technology and Society
- Travel and Holiday
- Visual Culture
- Browse content in Law
- Arbitration
- Browse content in Company and Commercial Law
- Commercial Law
- Company Law
- Browse content in Comparative Law
- Systems of Law
- Competition Law
- Browse content in Constitutional and Administrative Law
- Government Powers
- Judicial Review
- Local Government Law
- Military and Defence Law
- Parliamentary and Legislative Practice
- Construction Law
- Contract Law
- Browse content in Criminal Law
- Criminal Procedure
- Criminal Evidence Law
- Sentencing and Punishment
- Employment and Labour Law
- Environment and Energy Law
- Browse content in Financial Law
- Banking Law
- Insolvency Law
- History of Law
- Human Rights and Immigration
- Intellectual Property Law
- Browse content in International Law
- Private International Law and Conflict of Laws
- Public International Law
- IT and Communications Law
- Jurisprudence and Philosophy of Law
- Law and Politics
- Law and Society
- Browse content in Legal System and Practice
- Courts and Procedure
- Legal Skills and Practice
- Primary Sources of Law
- Regulation of Legal Profession
- Medical and Healthcare Law
- Browse content in Policing
- Criminal Investigation and Detection
- Police and Security Services
- Police Procedure and Law
- Police Regional Planning
- Browse content in Property Law
- Personal Property Law
- Study and Revision
- Terrorism and National Security Law
- Browse content in Trusts Law
- Wills and Probate or Succession
- Browse content in Medicine and Health
- Browse content in Allied Health Professions
- Arts Therapies
- Clinical Science
- Dietetics and Nutrition
- Occupational Therapy
- Operating Department Practice
- Physiotherapy
- Radiography
- Speech and Language Therapy
- Browse content in Anaesthetics
- General Anaesthesia
- Neuroanaesthesia
- Browse content in Clinical Medicine
- Acute Medicine
- Cardiovascular Medicine
- Clinical Genetics
- Clinical Pharmacology and Therapeutics
- Dermatology
- Endocrinology and Diabetes
- Gastroenterology
- Genito-urinary Medicine
- Geriatric Medicine
- Infectious Diseases
- Medical Oncology
- Medical Toxicology
- Pain Medicine
- Palliative Medicine
- Rehabilitation Medicine
- Respiratory Medicine and Pulmonology
- Rheumatology
- Sleep Medicine
- Sports and Exercise Medicine
- Clinical Neuroscience
- Community Medical Services
- Critical Care
- Emergency Medicine
- Forensic Medicine
- Haematology
- History of Medicine
- Browse content in Medical Dentistry
- Oral and Maxillofacial Surgery
- Paediatric Dentistry
- Restorative Dentistry and Orthodontics
- Surgical Dentistry
- Medical Ethics
- Browse content in Medical Skills
- Clinical Skills
- Communication Skills
- Nursing Skills
- Surgical Skills
- Medical Statistics and Methodology
- Browse content in Neurology
- Clinical Neurophysiology
- Neuropathology
- Nursing Studies
- Browse content in Obstetrics and Gynaecology
- Gynaecology
- Occupational Medicine
- Ophthalmology
- Otolaryngology (ENT)
- Browse content in Paediatrics
- Neonatology
- Browse content in Pathology
- Chemical Pathology
- Clinical Cytogenetics and Molecular Genetics
- Histopathology
- Medical Microbiology and Virology
- Patient Education and Information
- Browse content in Pharmacology
- Psychopharmacology
- Browse content in Popular Health
- Caring for Others
- Complementary and Alternative Medicine
- Self-help and Personal Development
- Browse content in Preclinical Medicine
- Cell Biology
- Molecular Biology and Genetics
- Reproduction, Growth and Development
- Primary Care
- Professional Development in Medicine
- Browse content in Psychiatry
- Addiction Medicine
- Child and Adolescent Psychiatry
- Forensic Psychiatry
- Learning Disabilities
- Old Age Psychiatry
- Psychotherapy
- Browse content in Public Health and Epidemiology
- Epidemiology
- Public Health
- Browse content in Radiology
- Clinical Radiology
- Interventional Radiology
- Nuclear Medicine
- Radiation Oncology
- Reproductive Medicine
- Browse content in Surgery
- Cardiothoracic Surgery
- Gastro-intestinal and Colorectal Surgery
- General Surgery
- Neurosurgery
- Paediatric Surgery
- Peri-operative Care
- Plastic and Reconstructive Surgery
- Surgical Oncology
- Transplant Surgery
- Trauma and Orthopaedic Surgery
- Vascular Surgery
- Browse content in Science and Mathematics
- Browse content in Biological Sciences
- Aquatic Biology
- Biochemistry
- Bioinformatics and Computational Biology
- Developmental Biology
- Ecology and Conservation
- Evolutionary Biology
- Genetics and Genomics
- Microbiology
- Molecular and Cell Biology
- Natural History
- Plant Sciences and Forestry
- Research Methods in Life Sciences
- Structural Biology
- Systems Biology
- Zoology and Animal Sciences
- Browse content in Chemistry
- Analytical Chemistry
- Computational Chemistry
- Crystallography
- Environmental Chemistry
- Industrial Chemistry
- Inorganic Chemistry
- Materials Chemistry
- Medicinal Chemistry
- Mineralogy and Gems
- Organic Chemistry
- Physical Chemistry
- Polymer Chemistry
- Study and Communication Skills in Chemistry
- Theoretical Chemistry
- Browse content in Computer Science
- Artificial Intelligence
- Computer Architecture and Logic Design
- Game Studies
- Human-Computer Interaction
- Mathematical Theory of Computation
- Programming Languages
- Software Engineering
- Systems Analysis and Design
- Virtual Reality
- Browse content in Computing
- Business Applications
- Computer Security
- Computer Games
- Computer Networking and Communications
- Digital Lifestyle
- Graphical and Digital Media Applications
- Operating Systems
- Browse content in Earth Sciences and Geography
- Atmospheric Sciences
- Environmental Geography
- Geology and the Lithosphere
- Maps and Map-making
- Meteorology and Climatology
- Oceanography and Hydrology
- Palaeontology
- Physical Geography and Topography
- Regional Geography
- Soil Science
- Urban Geography
- Browse content in Engineering and Technology
- Agriculture and Farming
- Biological Engineering
- Civil Engineering, Surveying, and Building
- Electronics and Communications Engineering
- Energy Technology
- Engineering (General)
- Environmental Science, Engineering, and Technology
- History of Engineering and Technology
- Mechanical Engineering and Materials
- Technology of Industrial Chemistry
- Transport Technology and Trades
- Browse content in Environmental Science
- Applied Ecology (Environmental Science)
- Conservation of the Environment (Environmental Science)
- Environmental Sustainability
- Environmentalist Thought and Ideology (Environmental Science)
- Management of Land and Natural Resources (Environmental Science)
- Natural Disasters (Environmental Science)
- Nuclear Issues (Environmental Science)
- Pollution and Threats to the Environment (Environmental Science)
- Social Impact of Environmental Issues (Environmental Science)
- History of Science and Technology
- Browse content in Materials Science
- Ceramics and Glasses
- Composite Materials
- Metals, Alloying, and Corrosion
- Nanotechnology
- Browse content in Mathematics
- Applied Mathematics
- Biomathematics and Statistics
- History of Mathematics
- Mathematical Education
- Mathematical Finance
- Mathematical Analysis
- Numerical and Computational Mathematics
- Probability and Statistics
- Pure Mathematics
- Browse content in Neuroscience
- Cognition and Behavioural Neuroscience
- Development of the Nervous System
- Disorders of the Nervous System
- History of Neuroscience
- Invertebrate Neurobiology
- Molecular and Cellular Systems
- Neuroendocrinology and Autonomic Nervous System
- Neuroscientific Techniques
- Sensory and Motor Systems
- Browse content in Physics
- Astronomy and Astrophysics
- Atomic, Molecular, and Optical Physics
- Biological and Medical Physics
- Classical Mechanics
- Computational Physics
- Condensed Matter Physics
- Electromagnetism, Optics, and Acoustics
- History of Physics
- Mathematical and Statistical Physics
- Measurement Science
- Nuclear Physics
- Particles and Fields
- Plasma Physics
- Quantum Physics
- Relativity and Gravitation
- Semiconductor and Mesoscopic Physics
- Browse content in Psychology
- Affective Sciences
- Clinical Psychology
- Cognitive Neuroscience
- Cognitive Psychology
- Criminal and Forensic Psychology
- Developmental Psychology
- Educational Psychology
- Evolutionary Psychology
- Health Psychology
- History and Systems in Psychology
- Music Psychology
- Neuropsychology
- Organizational Psychology
- Psychological Assessment and Testing
- Psychology of Human-Technology Interaction
- Psychology Professional Development and Training
- Research Methods in Psychology
- Social Psychology
- Browse content in Social Sciences
- Browse content in Anthropology
- Anthropology of Religion
- Human Evolution
- Medical Anthropology
- Physical Anthropology
- Regional Anthropology
- Social and Cultural Anthropology
- Theory and Practice of Anthropology
- Browse content in Business and Management
- Business Strategy
- Business History
- Business Ethics
- Business and Government
- Business and Technology
- Business and the Environment
- Comparative Management
- Corporate Governance
- Corporate Social Responsibility
- Entrepreneurship
- Health Management
- Human Resource Management
- Industrial and Employment Relations
- Industry Studies
- Information and Communication Technologies
- International Business
- Knowledge Management
- Management and Management Techniques
- Operations Management
- Organizational Theory and Behaviour
- Pensions and Pension Management
- Public and Nonprofit Management
- Strategic Management
- Supply Chain Management
- Browse content in Criminology and Criminal Justice
- Criminal Justice
- Criminology
- Forms of Crime
- International and Comparative Criminology
- Youth Violence and Juvenile Justice
- Development Studies
- Browse content in Economics
- Agricultural, Environmental, and Natural Resource Economics
- Asian Economics
- Behavioural Finance
- Behavioural Economics and Neuroeconomics
- Econometrics and Mathematical Economics
- Economic Systems
- Economic Methodology
- Economic History
- Economic Development and Growth
- Financial Markets
- Financial Institutions and Services
- General Economics and Teaching
- Health, Education, and Welfare
- History of Economic Thought
- International Economics
- Labour and Demographic Economics
- Law and Economics
- Macroeconomics and Monetary Economics
- Microeconomics
- Public Economics
- Urban, Rural, and Regional Economics
- Welfare Economics
- Browse content in Education
- Adult Education and Continuous Learning
- Care and Counselling of Students
- Early Childhood and Elementary Education
- Educational Equipment and Technology
- Educational Strategies and Policy
- Higher and Further Education
- Organization and Management of Education
- Philosophy and Theory of Education
- Schools Studies
- Secondary Education
- Teaching of a Specific Subject
- Teaching of Specific Groups and Special Educational Needs
- Teaching Skills and Techniques
- Browse content in Environment
- Applied Ecology (Social Science)
- Climate Change
- Conservation of the Environment (Social Science)
- Environmentalist Thought and Ideology (Social Science)
- Natural Disasters (Environment)
- Social Impact of Environmental Issues (Social Science)
- Browse content in Human Geography
- Cultural Geography
- Economic Geography
- Political Geography
- Browse content in Interdisciplinary Studies
- Communication Studies
- Museums, Libraries, and Information Sciences
- Browse content in Politics
- African Politics
- Asian Politics
- Chinese Politics
- Comparative Politics
- Conflict Politics
- Elections and Electoral Studies
- Environmental Politics
- European Union
- Foreign Policy
- Gender and Politics
- Human Rights and Politics
- Indian Politics
- International Relations
- International Organization (Politics)
- International Political Economy
- Irish Politics
- Latin American Politics
- Middle Eastern Politics
- Political Methodology
- Political Communication
- Political Philosophy
- Political Sociology
- Political Theory
- Political Behaviour
- Political Economy
- Political Institutions
- Politics and Law
- Public Administration
- Public Policy
- Quantitative Political Methodology
- Regional Political Studies
- Russian Politics
- Security Studies
- State and Local Government
- UK Politics
- US Politics
- Browse content in Regional and Area Studies
- African Studies
- Asian Studies
- East Asian Studies
- Japanese Studies
- Latin American Studies
- Middle Eastern Studies
- Native American Studies
- Scottish Studies
- Browse content in Research and Information
- Research Methods
- Browse content in Social Work
- Addictions and Substance Misuse
- Adoption and Fostering
- Care of the Elderly
- Child and Adolescent Social Work
- Couple and Family Social Work
- Developmental and Physical Disabilities Social Work
- Direct Practice and Clinical Social Work
- Emergency Services
- Human Behaviour and the Social Environment
- International and Global Issues in Social Work
- Mental and Behavioural Health
- Social Justice and Human Rights
- Social Policy and Advocacy
- Social Work and Crime and Justice
- Social Work Macro Practice
- Social Work Practice Settings
- Social Work Research and Evidence-based Practice
- Welfare and Benefit Systems
- Browse content in Sociology
- Childhood Studies
- Community Development
- Comparative and Historical Sociology
- Economic Sociology
- Gender and Sexuality
- Gerontology and Ageing
- Health, Illness, and Medicine
- Marriage and the Family
- Migration Studies
- Occupations, Professions, and Work
- Organizations
- Population and Demography
- Race and Ethnicity
- Social Theory
- Social Movements and Social Change
- Social Research and Statistics
- Social Stratification, Inequality, and Mobility
- Sociology of Religion
- Sociology of Education
- Sport and Leisure
- Urban and Rural Studies
- Browse content in Warfare and Defence
- Defence Strategy, Planning, and Research
- Land Forces and Warfare
- Military Administration
- Military Life and Institutions
- Naval Forces and Warfare
- Other Warfare and Defence Issues
- Peace Studies and Conflict Resolution
- Weapons and Equipment

- < Previous chapter

16 Case-based discussions
- Published: March 2009
- Cite Icon Cite
- Permissions Icon Permissions
Case-based discussion questions
Abdominal pain, bleeding, and rape.
An 18-year-old attends the emergency department with abdominal pain and vaginal bleeding. Her last period was 1 week prior and she has not had intercourse since then. When taking the history she reports an alleged vaginal rape by a stranger 5 h prior to presenting. You are the first person she has told and she becomes very distressed
Case continued: she decides she does want police involvement. She is not using any regular contraception. She says the assailant ejaculated inside her vagina without a condom. He was a white male aged about 30 years. She has not been bitten and has noticed no other injuries.
Unprotected sex
A 22-year-old attends her local family planning clinic requesting the ‘morning after’ pill. She had unprotected sex 5 days before. The first day of her last period was 22 days ago. She has had three episodes of unprotected sex since her period and has not taken emergency contraception in this cycle. Her cycle is regular and 32 days long.
Signed in as
Institutional accounts.
- GoogleCrawler [DO NOT DELETE]
- Google Scholar Indexing
Personal account
- Sign in with email/username & password
- Get email alerts
- Save searches
- Purchase content
- Activate your purchase/trial code
Institutional access
- Sign in with a library card Sign in with username/password Recommend to your librarian
- Institutional account management
- Get help with access
Access to content on Oxford Academic is often provided through institutional subscriptions and purchases. If you are a member of an institution with an active account, you may be able to access content in one of the following ways:
IP based access
Typically, access is provided across an institutional network to a range of IP addresses. This authentication occurs automatically, and it is not possible to sign out of an IP authenticated account.
Sign in through your institution
Choose this option to get remote access when outside your institution. Shibboleth/Open Athens technology is used to provide single sign-on between your institution’s website and Oxford Academic.
- Click Sign in through your institution.
- Select your institution from the list provided, which will take you to your institution's website to sign in.
- When on the institution site, please use the credentials provided by your institution. Do not use an Oxford Academic personal account.
- Following successful sign in, you will be returned to Oxford Academic.
If your institution is not listed or you cannot sign in to your institution’s website, please contact your librarian or administrator.
Sign in with a library card
Enter your library card number to sign in. If you cannot sign in, please contact your librarian.
Society Members
Society member access to a journal is achieved in one of the following ways:
Sign in through society site
Many societies offer single sign-on between the society website and Oxford Academic. If you see ‘Sign in through society site’ in the sign in pane within a journal:
- Click Sign in through society site.
- When on the society site, please use the credentials provided by that society. Do not use an Oxford Academic personal account.
If you do not have a society account or have forgotten your username or password, please contact your society.
Sign in using a personal account
Some societies use Oxford Academic personal accounts to provide access to their members. See below.
A personal account can be used to get email alerts, save searches, purchase content, and activate subscriptions.
Some societies use Oxford Academic personal accounts to provide access to their members.
Viewing your signed in accounts
Click the account icon in the top right to:
- View your signed in personal account and access account management features.
- View the institutional accounts that are providing access.
Signed in but can't access content
Oxford Academic is home to a wide variety of products. The institutional subscription may not cover the content that you are trying to access. If you believe you should have access to that content, please contact your librarian.
For librarians and administrators, your personal account also provides access to institutional account management. Here you will find options to view and activate subscriptions, manage institutional settings and access options, access usage statistics, and more.
Our books are available by subscription or purchase to libraries and institutions.
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Rights and permissions
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
- Not an Guest! Login
- Forgot Password
- CASE REPORTS
Wilson’s Disease Diagnosed Postnatally Due to Neurological Manifestation
Pregnancy and its outcome in a rare case of combined protein c and protein s deficiency with severe adenomyosis case, spontaneous ohss in a young adolescent: a diagnostic dilemma, laparoscopic approach for recurrent huge vulval mass, pregnancy in a persistent vegetative state: a management dilemma. case report, literature review and ethical concerns.
Sujata Siwatch 1 • Minakshi Rohilla 1 • Apinderpreet Singh 2 • Chirag Ahuja 3 • Kajal Jain 4 • Vanita Jain 1
A woman who developed a persistent vegetative state in the late first trimester after an arterio-venous fistula (AVF) bleed in the brain presented at 12 weeks period of gestation. The difficult clinical and ethical management issues faced include whether to continue pregnancy, antenatal care and planning for delivery. Multidisciplinary team management along with a family centred approach helped in planning and continuing the pregnancy that resulted in a successful fetal outcome.
Keywords: Pregnancy • Persistent vegetative state • Coma • Ethical issues
Abbreviations:
AV arterio-venous ICH intracranial hemorrhage ECA external carotid artery ICA internal carotid artery MCA middle cerebral artery DSA digital subtraction angiography PVS persistent vegetative state
Inflammatory Myofibroblastic Tumour at Episiotomy Site: A Rare Case Report with Review of Literature
Meenal Bhati 1 • Meenakshi Gothwal 2 • Pratibha Singh 3 • Garima Yadav 2
An inflammatory myofibroblastic tumour (IMT) is a rare mesenchymal neoplasm which was earlier considered under the broad category of inflammatory pseudotumor. It can arise from various anatomic location, out of all lung is the most common site. In our case a 27 years old female presented in our OPD with a mass arising from the episiotomy scar site in the vagina. The histopathological examination showed spindle-shaped cells in fascicles with inflamed granulation tissue with dense mixed inflammation. Immunohistochemistry test showed immunoreactivity for Smooth muscle actin (SMA) and are focally immunoreactive for Bcl2 and Desmin, negative for CK, CD34 and S100 protein. We framed our diagnosis of an inflammatory myofibroblastic tumour of the episiotomy site. However, female genital tract IMT's are rare; to the best of our knowledge, there are no reported cases of IMT involving episiotomy site.
Pancreatitis in Pregnancy: Case Series for 5 Years
Chandrakala Magudapathi 1 • Sudha Shanthi 2 • R. Palanisamy 3
Background To study the course of pancreatitis in pregnant women and demonstrate that early diagnosis and conservative management leads to good maternal and perinatal outcome.
Methods: This article is a retrospective case series study. Six patients with acute pancreatitis during pregnancy were seen in a tertiary referral based obstetric practice at our department in the last 5 years. One of them had gallstones, one hyperlipidemia, one Diabetes and one miliary tuberculosis on ATT . Conservative treatment was instituted for pancreatitis. All of them were followed at least six weeks post-partum.
Results: There was no maternal mortality and perinatal mortality. Acute pancreatitis occurred in both primipara and multipara patients. Preterm labor was a complication in most of our cases complicated by acute pancreatitis. Most patients experienced relief from the pancreatitis soon after delivery. One patient underwent cesarean section due to fetal distress all the other 5 patients had vaginal delivery. One patient had Pseudopancreatic cyst and had a morbid postpartum period.
Conclusion: Pancreatitis is a rare event in pregnancy, approximately 3 in 10,000 pregnancies. It is most often acute and related to gallstones but nonbiliary causes should be sought because they are associated with worse outcomes. Although acute pancreatitis is a rare complication of pregnancy with 50% maternal and 70 % perinatal mortality early and appropriate treatment is of utmost importance to improve the outcome.
Ovarian Follicle: Twirling Microfilaria’s New Abode
Sachin Khanduri 1 · Namrata Nigam 2 · Mazhar Khan 1 · Anvisha Shukla 1 · Ekta Tyagi 1 · Tariq Ahmad Imam 1 · Shobha Khanduri 3
Filariasis is parasitic disease with significant morbidity and socio-economic implications. Its uncommon presentation in female genital organs and rarer presentation in ovarian follicles pose a major diagnostic problem even in endemic regions.As in recent times, there is increase in travel and immigration ,physicians need to be familiar with cases not only endemic to their region but to non endemic diseases as well.Herein ,we report a case of a 26 year old female patient who presented with chronic pelvic pain and polymenorrhoea. Transvaginal ultrasonography revealed microfilariae in ovarian follicular fluid which led to correct diagnosis. This case report sheds light on uncommon presentation of filariasis which needs to be considered for correct diagnosis in endemic as well as non-endemic regions.
Effective Management of Early Cervical Pregnancy with Bilateral Uterine Artery Embolization Followed by Immediate Evacuation and Curettage: A Case Report
Pregnancy in a rare case of intracranial rosai dorfman disease (rdd).
Shashikala Ksheerasagar 1,2 · N. Venkatesh 1 · Niti Raizada 1 · K. M. Prathima 1 · Ravindra B. Kamble 1 · K. Srinivas 1 · M. A. Suzi Jacklin 1 · B. A. Chandramouli 1
We report an extremely rare case of spontaneous pregnancy in a 38 year women following chemotherapy for Rosai-Dorfman Disease (Rosai-dorfman Disease). What made the case more interesting was the challenges that obstetric team faced managing the patient in the presence of co-morbidities like Gestational Diabetes Mellitus , anemia , sub clinical hypothyroidism , allergic bronchitis , progressive symptoms of Rosai-Dorfman Disease like diplopia and cerebellar ataxia
Granulosa Cell Tumor of the Ovary Accompanying with Ollier’s Disease: First Case of Contralateral Presentations
Amirmohsen Jalaeefar 1 · Mohammad Shirkhoda 1 · Amirsina Sharifi 2 · Mohsen Sfandbod 3
Objective: Granulosa cell tumor (GCT) is a rare entity of ovarian malignancies. Juvenile GCT is considered a malignant tumor with an indolent course and tendency toward late recurrence. However, the association of this tumor and multiple enchondromas has been reported.
Case Presentation: A 17-year-old female with abnormal uterine bleeding was referred to our center. Ultrasonographic evaluation revealed a mass with origin in right ovary. Patient was worked up to undergo salpingo-oophorectomy, she felt a dull pain in her left lower limb. X-ray imaging was indicative for Ollier’s disease at the distal part of femur and proximal part of tibia. Postoperative pathological review was compatible with juvenile granulosa tumor of the right ovary.
Conclusion: This case was the first of its kind that ovarian tumor was contralateral to the side involved by enchondromatosis.
Ogilvie Syndrome with Caecal Perforation After Caesarean Section
Osseous metaplasia of the vaginal vault: a case report, heterotopic quadruplet pregnancy after icsi conception.
Background : Heterotopic pregnancy (HP) is a condition characterized by the coexistence of multiple fetuses at two or more implantation sites. It occurs in 1% of pregnancies after assisted reproductive techniques (ART). Presence of triplet intrauterine pregnancy with ectopic gestational sac is one of the rarest forms of HP. Ectopic pregnancy is implanted in the ampullary segment of the fallopian tube in 80% of cases. Most of the patients present with acute abdominal symptoms due to rupture of the tube. Case Presentation This article reports a case of quadruplet heterotopic pregnancy after intracytoplasmic sperm injection (ICSI) with an ampullary ectopic pregnancy and intrauterine triplet pregnancies. The ruptured ampullary pregnancy was emergently managed by right salpingectomy. This was followed by embryo reduction at 12 ? 6 weeks and successful outcome of intrauterine twin pregnancy.
A Rare Case of Adenoma Malignum: Preparing for the Unforeseen
Gayathri Dinesh Kamath 1 • Aditi Bhatt 1 • Veena Ramaswamy 1
Gonadal Vein Graft for Maintaining Renal Circulation After a Complication During Para-Aortic Nodal Dissection: A Case Report
Pesona Grace Lucksom 1 • Jaydip Bhaumik 1 • Gautam Biswas 2 • Sujoy Gupta 3 • Basumita Chakraborti 1
A 39 year old female underwent staging laparotomy for carcinoma endometrium. During para aortic node dissection the left renal vein (LRV) was accidentally injured. The patency of the LRV after rent repair was not adequate for functioning of the left kidney. Nepherectomy was considered but plans for saving the kidney was discussed by the joint team of surgeons. The venous blood of the left kidney was diverted through an anastomosis of the left gonadal vein with the venacava. Patency of the anastomosis was checked and was found to be adequate for keeping the left kidney functional. Doppler of the renal veins done on post-operative day three was normal and she was fit for discharge on day four.
Benign Ovarian Edema Masquerading as Malignancy: A Case Report
Shalini Singh 1 • Kameswari Surampudi 1 • Meenakshi Swain 2
Solid ovarian masses in young age can pose significant diagnostic and therapeutic challenges to the clinician. A young 16 year old girl presented with irregular cycles, pain abdomen and reportedly bulky ovaries with calcifications. Examination was unremarkable. Ultrasound scan revealed bilateral complex ovarian masses suggestive of neoplasm. MRI confirmed a solid right ovarian mass with normal left ovary. Tumour markers were normal. Option of frozen section followed by complete surgery if malignant or two stage procedure including staging laparotomy and if necessary a second surgery were discussed. Parents opted for the latter. At midline laparotomy, free fluid from abdomen was sent for cytology. Right ovary was irregular and enlarged measuring 10 x 8 cm with unruptured white capsule and no torsion. Left ovary was normal. Right salpingo-oophorectomy with omental and peritoneal biopsies were performed. Cytology was benign and histopathology showed massive ovarian edema which was a surprise and relief. Massive ovarian edema is a unique condition with tumour like enlargement of the ovary mimicking neoplasm on imaging leading to overtreatment of patients. Knowledge of this condition allows for fertility sparing procedures.
Maternal Near-Miss: A Perimortem Caesarean Section Resulting in a Remarkable Foetomaternal Recovery in a Rural Tertiary Care Centre in Eastern India
Leiomyoma of urinary bladder in middle-aged female.
Bhushan Dodia 1 • Abhay Mahajan 1 • Dhruti Amlani 1 • Sandeep Bathe 1
Member Login
Your attention is required, important notice.

The case-control study: a primer for the obstetrician-gynecologist
Affiliation.
- 1 Department of Obstetrics and Gynecology, Women & Infants' Hospital, Brown University School of Medicine, Providence, Rhode Island.
- PMID: 8008310
Case-control studies begin at the end. Two groups of patients, those with disease (cases) and those without (controls), are compared to determine the degree of exposure to a presumed risk factor. This research method is commonly used to study rare diseases or diseases that take years to develop. If a higher proportion of cases than controls has the exposure of interest, the exposure may be associated with illness. The strength of this association is measured by an "odds ratio," which is a good proxy for a relative risk when the illness in question is infrequent. Although some case-control studies are easy to do, all are easy to do poorly, especially because of selection bias in the choice of controls. A greater familiarity with the case-control study should enable obstetrician-gynecologists to evaluate critically published studies using this research method.
Publication types
- Case-Control Studies*
- Cohort Studies
- Confounding Factors, Epidemiologic
- Data Interpretation, Statistical
- Gynecology / education*
- Obstetrics / education*
- Reproducibility of Results
- Research / education
- Research Design* / standards
- Risk Factors
- Selection Bias
- Time Factors
- Introduction
- Conclusions
- Article Information
Study measures reflect self-reported responses by postpartum individuals 12 to 14 months after having a live birth. Detailed survey questions are included in eTable 1 in Supplement 1 . Percentages and 95% CIs were weighted to be representative of the 7 sample jurisdictions and to account for the Postpartum Assessment of Health Survey and Pregnancy Risk and Monitoring System nonresponse and sampling design. Error bars indicate 95% CIs.
Study measures reflect self-reported responses by postpartum individuals 12 to 14 months after having a live birth. Odds ratios (ORs) and 95% CIs were weighted to be representative of the 7 sample jurisdictions and to account for the Postpartum Assessment of Health Survey and Pregnancy Risk and Monitoring System nonresponse and sampling design. P values indicate the statistical significance of differences in the odds of reporting any item on the Mistreatment by Care Providers During Childbirth scale relative to the reference group based on unadjusted survey-weighted logistic regressions. Only characteristics with statistically significant comparisons are shown. IPFV indicates intimate partner or family violence; LGBTQ, lesbian, gay, bisexual, transgender, queer; PHE, public health emergency; and SUD, substance use disorder.
a Before or during pregnancy.
eTable 1. Mistreatment by Care Providers in Childbirth (MCPC) Survey Instrument
eTable 2. Sample Characteristics by Jurisdiction and Rates of Any Mistreatment
eTable 3. Unadjusted Associations Between Any Mistreatment and Patient Characteristics
eTable 4. Percentage of Respondents Experiencing Any Mistreatment by Race-Ethnicity, Marital Status, Sexual Orientation, and Insurance Status, for Combinations With Sample Size n ≥ 10
eTable 5. Individual Types of Mistreatment by Patient Characteristics
Data Sharing Statement
See More About
Sign up for emails based on your interests, select your interests.
Customize your JAMA Network experience by selecting one or more topics from the list below.
- Academic Medicine
- Acid Base, Electrolytes, Fluids
- Allergy and Clinical Immunology
- American Indian or Alaska Natives
- Anesthesiology
- Anticoagulation
- Art and Images in Psychiatry
- Artificial Intelligence
- Assisted Reproduction
- Bleeding and Transfusion
- Caring for the Critically Ill Patient
- Challenges in Clinical Electrocardiography
- Climate and Health
- Climate Change
- Clinical Challenge
- Clinical Decision Support
- Clinical Implications of Basic Neuroscience
- Clinical Pharmacy and Pharmacology
- Complementary and Alternative Medicine
- Consensus Statements
- Coronavirus (COVID-19)
- Critical Care Medicine
- Cultural Competency
- Dental Medicine
- Dermatology
- Diabetes and Endocrinology
- Diagnostic Test Interpretation
- Drug Development
- Electronic Health Records
- Emergency Medicine
- End of Life, Hospice, Palliative Care
- Environmental Health
- Equity, Diversity, and Inclusion
- Facial Plastic Surgery
- Gastroenterology and Hepatology
- Genetics and Genomics
- Genomics and Precision Health
- Global Health
- Guide to Statistics and Methods
- Hair Disorders
- Health Care Delivery Models
- Health Care Economics, Insurance, Payment
- Health Care Quality
- Health Care Reform
- Health Care Safety
- Health Care Workforce
- Health Disparities
- Health Inequities
- Health Policy
- Health Systems Science
- History of Medicine
- Hypertension
- Images in Neurology
- Implementation Science
- Infectious Diseases
- Innovations in Health Care Delivery
- JAMA Infographic
- Law and Medicine
- Leading Change
- Less is More
- LGBTQIA Medicine
- Lifestyle Behaviors
- Medical Coding
- Medical Devices and Equipment
- Medical Education
- Medical Education and Training
- Medical Journals and Publishing
- Mobile Health and Telemedicine
- Narrative Medicine
- Neuroscience and Psychiatry
- Notable Notes
- Nutrition, Obesity, Exercise
- Obstetrics and Gynecology
- Occupational Health
- Ophthalmology
- Orthopedics
- Otolaryngology
- Pain Medicine
- Palliative Care
- Pathology and Laboratory Medicine
- Patient Care
- Patient Information
- Performance Improvement
- Performance Measures
- Perioperative Care and Consultation
- Pharmacoeconomics
- Pharmacoepidemiology
- Pharmacogenetics
- Pharmacy and Clinical Pharmacology
- Physical Medicine and Rehabilitation
- Physical Therapy
- Physician Leadership
- Population Health
- Primary Care
- Professional Well-being
- Professionalism
- Psychiatry and Behavioral Health
- Public Health
- Pulmonary Medicine
- Regulatory Agencies
- Reproductive Health
- Research, Methods, Statistics
- Resuscitation
- Rheumatology
- Risk Management
- Scientific Discovery and the Future of Medicine
- Shared Decision Making and Communication
- Sleep Medicine
- Sports Medicine
- Stem Cell Transplantation
- Substance Use and Addiction Medicine
- Surgical Innovation
- Surgical Pearls
- Teachable Moment
- Technology and Finance
- The Art of JAMA
- The Arts and Medicine
- The Rational Clinical Examination
- Tobacco and e-Cigarettes
- Translational Medicine
- Trauma and Injury
- Treatment Adherence
- Ultrasonography
- Users' Guide to the Medical Literature
- Vaccination
- Venous Thromboembolism
- Veterans Health
- Women's Health
- Workflow and Process
- Wound Care, Infection, Healing
Get the latest research based on your areas of interest.
Others also liked.
- Download PDF
- X Facebook More LinkedIn
Liu C , Underhill K , Aubey JJ , Samari G , Allen HL , Daw JR. Disparities in Mistreatment During Childbirth. JAMA Netw Open. 2024;7(4):e244873. doi:10.1001/jamanetworkopen.2024.4873
Manage citations:
© 2024
- Permissions
Disparities in Mistreatment During Childbirth
- 1 Department of Health Policy and Management, Columbia University Mailman School of Public Health, New York, New York
- 2 Cornell Law School, Ithaca, New York
- 3 Department of Obstetrics and Gynecology, NewYork-Presbyterian/Columbia University Medical Center, New York, New York
- 4 Department of Population and Public Health Sciences, Keck School of Medicine, University of Southern California, Los Angeles
- 5 Columbia University School of Social Work, New York, New York
Question How often do birthing individuals in the US experience mistreatment by health care professionals during childbirth?
Findings In this cross-sectional study, 13.4% of birthing individuals reported experiencing mistreatment during childbirth. Individuals at higher risk included those who were unmarried; were Medicaid insured; were lesbian, gay, bisexual, transgender, queer identifying; had obesity; had a history of substance use disorder, mood disorders, or intimate partner or family violence; or had an unplanned cesarean birth.
Meaning These results suggest that structural social stigmas permeate the birth experience and shape how care is received, highlighting the need for patient-centered interventions to improve childbirth experiences.
Importance Lack of respectful maternity care may be a key factor associated with disparities in maternal health. However, mistreatment during childbirth has not been widely documented in the US.
Objectives To estimate the prevalence of mistreatment by health care professionals during childbirth among a representative multistate sample and to identify patient characteristics associated with mistreatment experiences.
Design, Setting, and Participants This cross-sectional study used representative survey data collected from respondents to the 2020 Pregnancy Risk and Monitoring System in 6 states and New York City who had a live birth in 2020 and participated in the Postpartum Assessment of Health Survey at 12 to 14 months’ post partum. Data were collected from January 1, 2021, to March 31, 2022.
Exposures Demographic, social, clinical, and birth characteristics that have been associated with patients’ health care experiences.
Main Outcomes and Measures Any mistreatment during childbirth, as measured by the Mistreatment by Care Providers in Childbirth scale, a validated measure of self-reported experiences of 8 types of mistreatment. Survey-weighted rates of any mistreatment and each mistreatment indicator were estimated, and survey-weighted logistic regression models estimated odds ratios (ORs) and 95% CIs.
Results The sample included 4458 postpartum individuals representative of 552 045 people who had live births in 2020 in 7 jurisdictions. The mean (SD) age was 29.9 (5.7) years, 2556 (54.4%) identified as White, and 2836 (58.8%) were commercially insured. More than 1 in 8 individuals (13.4% [95% CI, 11.8%-15.1%]) reported experiencing mistreatment during childbirth. The most common type of mistreatment was being “ignored, refused request for help, or failed to respond in a timely manner” (7.6%; 95% CI, 6.5%-8.9%). Factors associated with experiencing mistreatment included being lesbian, gay, bisexual, transgender, queer identifying (unadjusted OR [UOR], 2.3; 95% CI, 1.4-3.8), Medicaid insured (UOR, 1.4; 95% CI, 1.1-1.8), unmarried (UOR, 0.8; 95% CI, 0.6-1.0), or obese before pregnancy (UOR, 1.3; 95% CI, 1.0-1.7); having an unplanned cesarean birth (UOR, 1.6; 95% CI, 1.2-2.2), a history of substance use disorder (UOR, 2.6; 95% CI, 1.3-5.1), experienced intimate partner or family violence (UOR, 2.3; 95% CI, 1.3-4.2), mood disorder (UOR, 1.5; 95% CI, 1.1-2.2), or giving birth during the COVID-19 public health emergency (UOR, 1.5; 95% CI, 1.1-2.0). Associations of mistreatment with race and ethnicity, age, educational level, rural or urban geography, immigration status, and household income were ambiguous.
Conclusions and Relevance This cross-sectional study of individuals who had a live birth in 2020 in 6 states and New York City found that mistreatment during childbirth was common. There is a need for patient-centered, multifaceted interventions to address structural health system factors associated with negative childbirth experiences.
Discrimination and lack of respectful care are thought to be key factors associated with disparities in maternal mortality and morbidity in the US. 1 , 2 Negative experiences during childbirth can have long-term consequences for birthing individuals, including posttraumatic stress disorder, negative body image, feelings of dehumanization, and changes in future reproductive decisions. 3 - 7 However, experiences of mistreatment during childbirth have not been widely documented in the US. In 2019, the Giving Voice to Mothers (GVtM) Study developed the Mistreatment by Care Providers in Childbirth (MCPC) scale, the first patient-designed and validated measure of self-reported mistreatment during childbirth in the US, to our knowledge. 7 Based on a convenience sample of birthing individuals from marginalized groups, the GVtM study found that 17% experienced mistreatment. Rates were higher among members of racial and ethnic minority populations and individuals with low socioeconomic status. 7 In 2023, the Centers for Disease Control and Prevention (CDC) measured mistreatment among a convenience sample of mothers with children younger than 18 years; 20% reported mistreatment during pregnancy and delivery, with higher rates among Black (30%), Hispanic (29%), and publicly insured mothers (26%). 8
Although these studies suggest that mistreatment during pregnancy and delivery is common in the US, both relied on convenience samples. The present study uses a large, representative, multistate sample to (1) estimate the prevalence of mistreatment by health care professionals during childbirth, (2) identify the most common types of mistreatment, and (3) identify the demographic, social, and clinical characteristics associated with mistreatment experiences.
For this cross-sectional study, we used data from the 2020 Postpartum Assessment of Health Survey (PAHS), a multistate survey of birthing individuals 12 to 14 months after a live birth in 6 states (Kansas, Michigan, New Jersey, Pennsylvania, Utah, and Virginia) and New York City. 9 The design of PAHS builds on the CDC Pregnancy Risk and Monitoring System (PRAMS). The participating jurisdictions were selected based on PRAMS sample size, meeting CDC PRAMS response rate thresholds, and their willingness and capacity to collaborate in the PAHS. 9 Each year, the PRAMS sampling frame comprises a stratified random sample of live births drawn monthly from state or city birth certificates. 10 Individuals in the 2020 PRAMS sampling frame gave birth between January and December 2020 and completed the PRAMS survey from 2 to 6 months post partum. PRAMS respondents were given the option to opt out of being contacted again for the PAHS from 12 to 14 months post partum. Verbal or written consent was obtained depending on the mode of the survey response. PAHS recruitment and data collection then occurred from January 1, 2021, to March 31, 2022. Of those contacted for the PAHS (6021 of 8473; 71.1% of 2020 PRAMS respondents), 4598 completed the survey (76.4% response rate). The PAHS was offered in English and Spanish. Individual-level PAHS responses were linked to PRAMS responses and birth certificate variables. This study was approved by the institutional review boards of the CDC, Columbia University, Rutgers University, and each local jurisdiction. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology ( STROBE ) reporting guideline.
The primary outcome was any mistreatment. The MCPC scale was developed and validated using a community-based participatory research process with targeted recruitment of pregnant individuals from racial and ethnic minority populations. 7 PAHS respondents were asked to think back to their birthing experience in the previous year to recall whether they had experienced any of 7 issues or behaviors from health care professionals during childbirth (eTable 1 in Supplement 1 ), which included physical abuse, verbal abuse (shouted at or scolded, or threatened), neglect, abandonment, lack of informed consent, and breach of confidentiality. Although not included in the MCPC scale, PAHS respondents could also indicate that they experienced any other mistreatment. Any mistreatment was coded as 1 if respondents answered yes to any of the 7 issues or any other mistreatment and 0 if respondents answered no to all.
We measured individual-level demographic, social, and clinical characteristics that have been associated with patients’ perinatal or other health care experiences in prior research. Self-reported race and ethnicity, which was shown to be a factor associated with mistreatment in the GVtM study, was measured on the PAHS. Respondents could choose between 8 categories: Asian; Black; Hispanic or Latinx; Native Hawaiian or Pacific Islander; Native American or Alaska Native; Southwest Asian, Middle Eastern, or North African; White; and multiple minoritized races. Most respondents (95.0% [4368 of 4596]) selected a single race and ethnicity category. We categorized individuals who selected 2 races and ethnicities, including White, as the other race and ethnicity, and those who selected multiple races and ethnicities other than White as “multiple minoritized races.”
Other sociodemographic characteristics included age; lesbian, gay, bisexual, transgender, queer (LGBTQ) identity; marital or domestic partner status; educational level; primary language; household income as a percentage of the 2021 federal poverty level; immigration status (for all jurisdictions except New York City); insurance coverage; and rural or nonrural geography (based on 2013 Rural-Urban Continuum Codes). 11 Missingness for sociodemographic variables measured in the PAHS was low (range, 0.1%-4.4%). For variables with an equivalent measure in the PRAMS or the birth certificate (race and ethnicity, age, marital status, educational level, income, and insurance at birth), we used these measures to impute the missing PAHS values.
We drew on prior studies of medical stigma and mistreatment to guide selection of other covariates. Intimate partner violence was associated with mistreatment in the GVtM study. 7 We therefore measured intimate partner or family violence (IPFV) during or 12 months before pregnancy by one’s husband, current or ex-partner, or another family member. Prior studies have shown that some physical and mental health conditions (eg, excess body weight and behavioral health disorders) carry stigmas that negatively shape health care professionals’ care and attitudes towards patients. 12 - 14 We measured obesity (body mass index ≥30 [calculated as weight in kilograms divided by height in meters squared]) prior to pregnancy and self-reported diagnosis of the following conditions before or during pregnancy: chronic medical conditions (asthma, diabetes, or hypertension), substance use disorder (SUD) or addiction (excluding smoking or tobacco use), and mood disorders (depression, anxiety, or another mood disorder).
Finally, we included birth characteristics that may shape an individual’s support, autonomy, and ability to participate in shared decision-making, 7 , 15 including parity; type of birth (vaginal, planned cesarean delivery, or unplanned cesarean delivery); a composite measure of higher-risk pregnancy (multiple births, preterm birth, gestational diabetes, or gestational hypertension); birth during the COVID-19 public health emergency (from March to December 2020); and presence or absence of a support person during childbirth (ie, no one, current partner or spouse, or others such as an ex-partner or ex-spouse or family members).
We estimated the survey-weighted rates of any mistreatment and each mistreatment indicator. We used survey-weighted logistic regression models to estimate odds ratios (ORs) and 95% CIs for the association between any mistreatment and patient characteristics. We aimed to identify the groups at highest risk of mistreatment; our goal was not to isolate the independent association of any one factor and mistreatment. We therefore did not adjust for covariates. Acknowledging that stigma and structural discrimination can result from multiple overlapping identities, 16 we further analyzed the intersectional associations of race and ethnicity with 3 demographic characteristics that had statistically significant associations with mistreatment: marital status, LGBTQ identity, and insurance coverage. To do so, we calculated survey-weighted rates of any mistreatment for groups defined by all 96 combinations of these 4 characteristics. We report rates only for the 29 groups with a total sample size of at least 10 individuals.
All estimates were weighted to be representative of live births in 2020 in the 7 jurisdictions. The PAHS weights accounted for the PRAMS stratified survey design, PRAMS nonresponse, and PAHS nonresponse. The PAHS weights were also calibrated to known population totals by maternal age, race and ethnicity, educational level, marital status, sampling strata, and infant birth weight based on 2020 live birth records in each jurisdiction. Missingness was low for the primary MCPC outcome (3.3%); thus, we conducted complete-case analysis. We conducted statistical tests using 2-sided tests and a significance level of P < .05. Analyses were performed using Stata, version 17 (StataCorp).
Among the sample of 4458 postpartum respondents, representative of 552 045 people who had live births in 2020 in 7 jurisdictions, the mean (SD) age was 29.9 (5.7) years, 2556 (54.4%) identified as White, followed by Hispanic or Latinx (790 [18.3%]), Black (620 [15.0%]), or Asian (319 [8.9%]) ( Table 1 ). Overall, 2695 respondents (58.8%) were between 25 and 34 years of age when they gave birth, 4089 (91.1%) identified as non-LGBTQ, 3571 (78.0%) were married or in a domestic partnership, 3270 (68.5%) had higher than a high school education, and 3787 (82.6%) primarily spoke English. At the time of childbirth, 2836 participants (58.8%) were commercially insured, 1479 (37.9%) were insured by Medicaid, and 142 (3.2%) were uninsured.
Figure 1 shows rates of mistreatment overall and by type of mistreatment. A total of 13.4% (95% CI, 11.8%-15.1%) of birthing individuals in 2020 reported experiencing some form of mistreatment during childbirth. Being “ignored, refused request for help, or failed to respond in a timely manner” was the most commonly reported type of mistreatment (7.6%; 95% CI, 6.5%-8.9%), followed by being “shouted at or scolded” by health care clinicians (4.1%; 95% CI, 3.3%-5.2%), any other mistreatment (2.7%; 95% CI, 2.1%-3.4%), and having health care clinicians threaten “to withhold treatment or force you to accept treatment that you did not want” (2.3%; 95% CI, 1.7%-3.1%). Mistreatment rates ranged from 9.0% (95% CI, 7.0%-11.5%) in Kansas to 16.9% (95% CI, 13.9%-20.3%) in New York City (eTable 2 in Supplement 1 ).
Rates of mistreatment varied widely by race and ethnicity; however, we did not detect statistically significant differences between White respondents and other groups ( Table 2 ; eTable 3 in Supplement 1 ). Respondents who were Southwest Asian, Middle Eastern, or North African reported the highest rates of mistreatment (33.7%; 95% CI, 13.1%-63.2%), followed by individuals of multiple minoritized races (16.9%; 95% CI, 6.4%-37.9%), Black respondents (15.9%; 95% CI, 12.1%-20.6%), White respondents (13.3%; 95% CI, 11.0%-16.0%), Native American or Alaska Native respondents (12.5%; 95% CI, 3.3%-37.5%), Asian respondents (11.5%; 95% CI, 8.2%-15.9%), and Hispanic or Latinx respondents (10.8%; 95% CI, 8.4%-13.8%) ( Table 1 ).
Figure 2 shows the unadjusted ORs (UORs) for patient characteristics that were statistically significantly associated with any mistreatment. We found that LGBTQ respondents were twice as likely to experience any mistreatment compared with non-LGBTQ respondents (UOR, 2.3; 95% CI, 1.4-3.8). Odds of mistreatment were higher among those nsured by Medicaid at birth (UOR, 1.4; 95% CI, 1.1-1.8) and lower among respondents who were married relative to those who were not married or in a domestic partnership (UOR, 0.8; 95% CI, 0.6-1.0). Spanish language speakers were less likely to report mistreatment relative to primary English speakers (UOR, 0.5; 95% CI, 0.3-0.9). We did not identify statistically significant differences in mistreatment rates by age, educational level, rural or urban geography, immigration status, or household income (eTable 3 in Supplement 1 ).
Individuals with a history of SUD (UOR, 2.6; 95% CI, 1.3-5.1) and IPFV (UOR, 2.3; 95% CI, 1.3-4.2) were nearly twice as likely to report mistreatment relative to those without SUD or IPFV ( Figure 2 ). Respondents with mood disorders before or during pregnancy (UOR, 1.5; 95% CI, 1.1-2.2) and those who were obese prior to pregnancy (UOR, 1.3; 95% CI, 1.0-1.7) were also more likely to report mistreatment. Respondents with an unplanned cesarean birth (UOR, 1.6; 95% CI, 1.2-2.2) reported higher rates of mistreatment relative to those with a vaginal birth, as did those who gave birth during the COVID-19 public health emergency (UOR, 1.5; 95% CI, 1.1-2.0). We did not find statistically significant associations of mistreatment with support at childbirth, chronic physical conditions, parity, or higher-risk pregnancy (eTable 3 in Supplement 1 ).
The most common forms of mistreatment differed by patient characteristics (eTable 5 in Supplement 1 ). For example, LGBTQ individuals reported statistically significantly higher rates of being “threatened [with] withhold[ing] treatment or forced to accept [unwanted] treatment” compared with non-LGBTQ individuals (11.1% vs 1.9%). Southwest Asian, Middle Eastern, or North African respondents were more likely to report that their “physical privacy was violated, such as being uncovered or having people in the delivery room” without consent relative to White respondents (21.3% vs. 1.2%).
eTable 4 in Supplement 1 shows the rates of mistreatment by combinations of race and ethnicity, marital status, LGBTQ identity, and insurance at time of birth among sample sizes larger than 10. Across Black and White groups, the combination of identifying as LGBTQ, being unmarried, and Medicaid insured was associated with higher risk of mistreatment, with more than one-third of respondents with these intersecting identities reporting mistreatment (Black, 36.1%; 95% CI, 11.7%-70.5%; White, 36.2%; 95% CI, 9.7%-75.0%). Southwest Asian, Middle Eastern, or North African respondents who were Medicaid insured, married or in a domestic partnership, and non-LGBTQ identifying reported the highest rate of mistreatment (55.9%; 95% CI, 13.1%-91.4%); however, the 95% CIs were wide.
Using multistate representative survey data, we found that mistreatment by health care professionals during childbirth is a common experience in the US, affecting more than 1 in 8 individuals with a live birth in 2020. The highest rates of mistreatment occurred among individuals who were unmarried; Medicaid insured; LGBTQ identifying; obese; had a history of SUD, mood disorders, or IPFV; and those who had an unplanned cesarean birth.
The overall prevalence of mistreatment in our sample is lower than in the GVtM study (17.4% in a convenience sample drawn from marginalized communities 7 ) and the CDC survey (20% in an online convenience sample of mothers with children <18 years). 8 However, the prevalence rate in our study of 13.4%—representative of all birthing individuals in 6 states and New York City—suggests a need for interventions to improve respectful maternity care in the US. Similar to the CDC study, which did not conduct statistical testing, we found higher rates of mistreatment among Black and multiracial individuals, as well as those with public insurance. Similarities with the GVtM study include statistically significantly higher mistreatment rates among individuals with a history of SUD or IPFV, those with public insurance, and those with unplanned cesarean births. We also isolated risk factors not previously explored, including LGBTQ identity, obesity, mood disorders, and marital status.
Many of our results suggest that a pervasive structural social stigma permeates the birth experience and shapes how care is received. 17 For example, we found that LGBTQ-identifying individuals were twice as likely to experience mistreatment, associated with higher rates of feeling forced to accept unwanted treatment or being denied wanted treatment. These findings align with prior work demonstrating poorer birth outcomes among sexual minority women, 18 as well as research linking stigma and heterosexist policies to minority stress and adverse health outcomes among LGBTQ-identifying individuals. 19
Similarly, our results follow prior research that has linked stigma, discrimination in health care settings, and adverse health outcomes for people with excess body weight, 20 , 21 birthing individuals who are unmarried, 22 - 25 and individuals of low socioeconomic status who are publicly insured. 26 The high prevalence of mistreatment experienced by Medicaid-insured birthing individuals warrants attention, and Medicaid program administrators could explore options such as coverage for doulas and financial incentives to encourage respectful maternity care.
Our findings of increased mistreatment among patients with SUD, mood disorders, and a history of IPFV are concerning. Recent research has found that homicide, suicide, and drug overdose are leading causes of deaths after childbirth. 27 , 28 Mistreatment during childbirth may deter patients from seeking potentially lifesaving health care services, such as care for mental health, substance use, and experiences of IPFV. Mistreatment could also affect patients’ trust in health care professionals and affiliated institutions, with adverse long-term consequences for care seeking, disclosure to clinicians, and uptake of social services. Health care professionals and institutions could adopt targeted interventions to address the needs of at-risk patient groups, to foster inclusive and justice-informed care, and to actively discourage, make visible, and remedy discrimination against patients. 29 , 30
Unlike the GVtM study, we did not identify statistically significant associations of mistreatment with younger age (17-25 years), race and ethnicity, nulliparity, or having a high-risk pregnancy. The GVtM study found that Black, Hispanic, and Indigenous mothers were statistically significantly more likely than White mothers to experience mistreatment. In our study, Southwest Asian, Middle Eastern, or North African respondents were the most likely to report mistreatment, followed by Black individuals and people of multiple minoritized races. Group differences, however, were not statistically significant, which may be due to sample size and use of survey weighting, which reduces statistical power but allows for representative estimates.
Numerous studies have identified control—namely, participation in shared decision-making and patient-clinician communication, including managing complications—as one of the most important factors in birth satisfaction. 4 , 31 , 32 The high rate of mistreatment experienced by respondents with unplanned cesarean births may reflect the dynamics of patient disempowerment, such as loss of autonomy and lack of communication regarding the indication for the procedure. Reported mistreatment among those with unplanned cesarean births was largely driven by high rates of being forced to accept unwanted treatment or being threatened with withholding treatment.
This study also points to some conditions of care settings that might be associated with mistreatment experiences. Mistreatment was statistically significantly higher among respondents who gave birth in the months after the onset of the COVID-19 pandemic, when health care systems and personnel were experiencing extreme stress and resource scarcity. Health care professionals, staff members, facilities, and patients were all navigating a lack of vaccines, a shortage in personal protective equipment, and significant changes to hospital visitor policies that reduced and, in some cases, briefly eliminated support persons during labor and childbirth. Other studies have shown how the health, social, and policy contexts of the pandemic were adversely associated with maternity care and patient experiences. 33 - 35 The high proportions of respondents in our study who reported being “ignored,” being “refused requests for help,” and being “shouted at or scolded” may partly reflect clinician burnout and resource constraints.
This study has some limitations. First, while our findings were representative of the 7 included jurisdictions, which comprised 19.8% of US births in 2020, 36 the results may not be generalizable to all US jurisdictions. Second, some null results, including comparisons by race and ethnicity and immigration status (which was not collected in New York City), could be due to insufficient statistical power rather than lack of true differences. Third, “any other mistreatment” was the third most common form of mistreatment, suggesting that some perceived mistreatment experiences are not captured by the options in the MCPC scale. Incorporating the MCPC scale in larger population surveys, such as the PRAMS, with a free text option, would allow for the tracking of mistreatment rates across jurisdictions and over time, the exploration of other forms of mistreatment, and the statistical power to better evaluate disparities. Fourth, the MCPC scale does not capture mistreatment during pregnancy. Fifth, all variables are self-reported and could be subject to recall or social desirability bias (eg, reporting of SUD). Sixth, PAHS participants gave birth in 2020. Mistreatment rates could vary outside of the pandemic context. Seventh, while the PAHS was offered in Spanish, we found considerably lower rates of mistreatment among Spanish-speaking individuals. This finding could reflect a real difference or differences in the interpretation of the MCPC scale, which was not specifically validated for Spanish populations.
In this cross-sectional study conducted in 6 states and New York City, we found that mistreatment during childbirth was a common experience. To our knowledge, evidence of effective interventions to improve respectful maternity care in the US is scant. There is a need for the development and evaluation of patient-centered, multifaceted interventions that address implicit biases, cultural competence, health care workforce conditions, the inclusivity of clinical settings, and other structural factors, including health system factors, to improve childbirth experiences.
Accepted for Publication: February 6, 2024.
Published: April 4, 2024. doi:10.1001/jamanetworkopen.2024.4873
Open Access: This is an open access article distributed under the terms of the CC-BY License . © 2024 Liu C et al. JAMA Network Open .
Corresponding Author: Chen Liu, MHS, Department of Health Policy and Management, Columbia University Mailman School of Public Health, 722 W 168th St, 4th Floor, New York, NY 10032 ( [email protected] ).
Author Contributions: Ms Liu had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Liu, Underhill, Allen, Daw.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: Liu, Allen.
Critical review of the manuscript for important intellectual content: All authors.
Statistical analysis: Liu, Samari, Daw.
Obtained funding: Underhill, Allen, Daw.
Administrative, technical, or material support: Samari, Daw.
Supervision: Underhill, Aubey, Allen, Daw.
Conflict of Interest Disclosures: Dr Allen reported receiving grants from the National Institute on Minority Health and Health Disparities during the conduct of the study and serving as a commissioner on the Medicaid and CHIP Payment and Access Commission. Dr Daw reported receiving grants from the National Institutes of Health outside the submitted work. No other disclosures were reported.
Funding/Support: This study was funded by Columbia World Projects, Columbia University.
Role of the Funder/Sponsor: The funding source had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclaimer: Any views or opinions expressed in this article are solely those of the authors, and no endorsement of these views or opinions by the authors’ institutions is expressed or implied.
Meeting Presentation: This study was presented at the Annual Research Meeting of AcademyHealth in 3 poster sessions over 2 days; June 25 and 26, 2023; Seattle, Washington.
Data Sharing Statement: See Supplement 2 .
Additional Contributions: The Postpartum Assessment of Health Survey (PAHS) was a collaboration between Columbia University and the following state and city partners: Kansas Department of Health and Environment, Michigan Department of Health and Human Services, New Jersey Department of Health, New York City Department of Health and Mental Hygiene, Pennsylvania Department of Health, Utah Department of Health and Human Services, and Virginia Department of Health. The PAHS operations were conducted by the Kansas Department of Health and Environment (for Kansas) and the Rutgers Bloustein Center for Survey Research (for the other 6 sites). We acknowledge and thank the Centers for Disease Control and Prevention for coordinating with the PAHS team.
- Register for email alerts with links to free full-text articles
- Access PDFs of free articles
- Manage your interests
- Save searches and receive search alerts
vNOTES surgical staging for endometrial carcinoma in overweight patients: a case series
- Gynecologic Oncology
- Published: 05 April 2024
Cite this article
- Luka Matak ORCID: orcid.org/0000-0001-9679-0198 1 ,
- Maša Šimičević 1 ,
- Branko Dukić 1 ,
- Magdalena Matak 2 &
- Jan Baekelandt 3
24 Accesses
Explore all metrics
The purpose of this study is to show the feasibility and surgical outcome of vNOTES retroperitoneal dissection and isolation of sentinel lymph nodes in overweight and obese patients with endometrial cancer.
Materials and methods
Four patients had undergone pelvic lymphadenectomy with a sentinel lymph node. Three patients were overweight, and one was obese with a BMI of 34.6 kg/m 2 . By using NMR mode sentinel lymph node was visualized, excised and marked separately for pathohistological analysis from the rest of the visualized lymph nodes that were then consecutively excised.
The mean number of overall excised lymph nodes was 12.5, and the mean number on the right side was 5.75 and 6.25 on the left side. There were no metastases verified in the pathohistological evaluation.
vNOTES retroperitoneal isolation of sentinel lymph nodes is good alternative and has its benefits, especially in overweight and obese patients with satisfying low intra- and postoperative complications.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
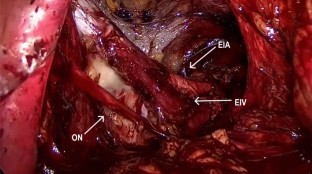
Data availability
Raw data were generated at General Hospital Zadar. Derived data supporting the findings of this study are available from the corresponding author (LM) on request.
Deng L, Liu Y, Yao Y, Deng Y, Tang S, Sun L, Wang Y (2023) Efficacy of vaginal natural orifice transluminal endoscopic sentinel lymph node biopsy for endometrial cancer: a prospective multicenter cohort study. Int J Surg (London, England) 109(10):2996–3002. https://doi.org/10.1097/JS9.0000000000000551
Article Google Scholar
Wang Y, Deng L, Tang S, Dou Y, Yao Y, Li Y, Deng Y, Chen Y, Liang Z (2021) vNOTES hysterectomy with sentinel lymph node mapping for endometrial cancer: description of technique and perioperative outcomes. J Minim Invasive Gynecol 28(6):1254–1261. https://doi.org/10.1016/j.jmig.2021.01.022
Article PubMed Google Scholar
Oh SH, Park SJ, Lee EJ, Yim GW, Kim HS (2019) Pelvic lymphadenectomy by vaginal natural orifice transluminal endoscopic surgery (vNOTES) for early-stage endometrial cancer. Gynecol Oncol 153(1):211–212. https://doi.org/10.1016/j.ygyno.2019.01.003
Huber D, Hurni Y (2022) Sentinel node biopsy for endometrial cancer by retroperitoneal transvaginal natural orifice transluminal endoscopic surgery: a preliminary study. Front Surg 9:907548. https://doi.org/10.3389/fsurg.2022.907548
Article PubMed PubMed Central Google Scholar
Baekelandt J, Stuart A (2023) A new anterior approach to vNOTES retroperitoneal sentinel node resection for endometrial cancer. Asian J Surg 46(12):5491–5492. https://doi.org/10.1016/j.asjsur.2023.07.127
Matanes E, Eisenberg N, Amajoud Z, Gupta V, Yasmeen A, Ismail S, Racovitan F, Raban O, Lau S, Salvador S, Gotlieb WH, Kogan L (2021) Sentinel lymph node sampling as an alternative to lymphadenectomy in patients with endometrial cancer and obesity. J Obstet Gynaecol Can 43(10):1136-1144.e1. https://doi.org/10.1016/j.jogc.2021.04.014
Mathey MP, Romito F, Huber DE (2022) Retroperitoneal sentinel lymph node biopsy by vaginally assisted natural orifices endoscopic transluminal endoscopic surgery in early stage endometrial cancer: description of technique and surgeon’s perspectives after the first experience. Case Rep Oncol 15(1):291–299. https://doi.org/10.1159/000523735
Eriksson AG, Montovano M, Beavis A, Soslow RA, Zhou Q, Abu-Rustum NR, Gardner GJ, Zivanovic O, Barakat RR, Brown CL, Levine DA, Sonoda Y, Leitao MM Jr, Jewell EL (2016) Impact of obesity on sentinel lymph node mapping in patients with newly diagnosed uterine cancer undergoing robotic surgery. Ann Surg Oncol 23(8):2522–2528. https://doi.org/10.1245/s10434-016-5134-2
Kaya C, Yıldız Ş, Alay İ, Aslan Ö, Aydıner İE, Yaşar L (2022) The comparison of surgical outcomes following laparoscopic hysterectomy and vNOTES hysterectomy in obese patients. J Investig Surg Off J Acad Surg Res 35(4):862–867. https://doi.org/10.1080/08941939.2021.1927262
Download references
The authors have not disclosed any funding.
Author information
Authors and affiliations.
Department of Obstetrics and Gynecology, General Hospital Zadar, Bože Peričića 5, 23000, Zadar, Croatia
Luka Matak, Maša Šimičević & Branko Dukić
Department of Dermatovenerology, General Hospital Zadar, Zadar, Croatia
Magdalena Matak
Department of Obstetrics and Gynaecology, Imelda Hospital, Bonheiden, Belgium
Jan Baekelandt
You can also search for this author in PubMed Google Scholar
Contributions
Investigation: Luka Matak, Jan Baekelandt. Conceptualization: Luka Matak, Jan Baekelandt. Methodology: Luka Matak. Supervision: Jan Baekelandt. Writing—original draft preparation: Luka Matak, Maša Šimičević. Validation: Luka Matak, Magdalena Matak. Data curation: Luka Matak, Branko Dukić. Writing—review and editing: Luka Matak, Branko Dukić.
Corresponding author
Correspondence to Luka Matak .
Ethics declarations
Conflict of interest.
Jan Baekelandt discloses consultancy for Applied Medical.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Matak, L., Šimičević, M., Dukić, B. et al. vNOTES surgical staging for endometrial carcinoma in overweight patients: a case series. Arch Gynecol Obstet (2024). https://doi.org/10.1007/s00404-024-07466-6
Download citation
Received : 02 January 2024
Accepted : 04 March 2024
Published : 05 April 2024
DOI : https://doi.org/10.1007/s00404-024-07466-6
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Endometrial cancer
- Find a journal
- Publish with us
- Track your research
- History, Facts & Figures
- YSM Dean & Deputy Deans
- YSM Administration
- Department Chairs
- YSM Executive Group
- YSM Board of Permanent Officers
- FAC Documents
- Current FAC Members
- Appointments & Promotions Committees
- Ad Hoc Committees and Working Groups
- Chair Searches
- Leadership Searches
- Organization Charts
- Faculty Demographic Data
- Professionalism Reporting Data
- 2022 Diversity Engagement Survey
- State of the School Archive
- Faculty Climate Survey: YSM Results
- Strategic Planning
- Mission Statement & Process
- Beyond Sterling Hall
- COVID-19 Series Workshops
- Previous Workshops
- Departments & Centers
- Find People
- Biomedical Data Science
- Health Equity
- Inflammation
- Neuroscience
- Global Health
- Diabetes and Metabolism
- Policies & Procedures
- Media Relations
- A to Z YSM Lab Websites
- A-Z Faculty List
- A-Z Staff List
- A to Z Abbreviations
- Dept. Diversity Vice Chairs & Champions
- Dean’s Advisory Council on Lesbian, Gay, Bisexual, Transgender, Queer and Intersex Affairs Website
- Minority Organization for Retention and Expansion Website
- Office for Women in Medicine and Science
- Committee on the Status of Women in Medicine Website
- Director of Scientist Diversity and Inclusion
- Diversity Supplements
- Frequently Asked Questions
- Recruitment
- By Department & Program
- News & Events
- Executive Committee
- Aperture: Women in Medicine
- Self-Reflection
- Portraits of Strength
- Mindful: Mental Health Through Art
- Event Photo Galleries
- Additional Support
- MD-PhD Program
- PA Online Program
- Joint MD Programs
- How to Apply
- Advanced Health Sciences Research
- Clinical Informatics & Data Science
- Clinical Investigation
- Medical Education
- Visiting Student Programs
- Special Programs & Student Opportunities
- Residency & Fellowship Programs
- Center for Med Ed
- Organizational Chart
- Committee Procedural Info (Login Required)
- Faculty Affairs Department Teams
- Recent Appointments & Promotions
- Academic Clinician Track
- Clinician Educator-Scholar Track
- Clinican-Scientist Track
- Investigator Track
- Traditional Track
- Research Ranks
- Instructor/Lecturer
- Social Work Ranks
- Voluntary Ranks
- Adjunct Ranks
- Other Appt Types
- Appointments
- Reappointments
- Transfer of Track
- Term Extensions
- Timeline for A&P Processes
- Interfolio Faculty Search
- Interfolio A&P Processes
- Yale CV Part 1 (CV1)
- Yale CV Part 2 (CV2)
- Samples of Scholarship
- Teaching Evaluations
- Letters of Evaluation
- Dept A&P Narrative
- A&P Voting
- Faculty Affairs Staff Pages
- OAPD Faculty Workshops
- Leadership & Development Seminars
- List of Faculty Mentors
- Incoming Faculty Orientation
- Faculty Onboarding
- Past YSM Award Recipients
- Past PA Award Recipients
- Past YM Award Recipients
- International Award Recipients
- Nominations Calendar
- OAPD Newsletter
- Fostering a Shared Vision of Professionalism
- Academic Integrity
- Addressing Professionalism Concerns
- Consultation Support for Chairs & Section Chiefs
- Policies & Codes of Conduct
- Health & Well-being
- First Fridays
- Fund for Physician-Scientist Mentorship
- Grant Library
- Grant Writing Course
- Mock Study Section
- Research Paper Writing
- Funding Opportunities
- Join Our Voluntary Faculty
- Faculty Resources
- Research by Keyword
- Research by Department
- Research by Global Location
- Translational Research
- Research Cores & Services
- Program for the Promotion of Interdisciplinary Team Science (POINTS)
- CEnR Steering Committee
- Experiential Learning Subcommittee
- Goals & Objectives
- Embryonic Stem Cell Research Oversight
- COVID-19 Vaccinations in CT
- COVID-19 in Connecticut Schools
- Connecticut Towns COVID-19 Impact Dashboard
- Connecticut Town 14-Day Cases Time Lapse
- CT Correctional Facilities with COVID Cases Dashboard
- Connecticut COVID Presence Map
- CT Nursing Homes with COVID-19 Cases
- U.S. COVID Presence Map
- COVID-19 Case Density by US County
- Global Cases Dashboard
- Time-Lapse of Global Spread
- US Racial and Ethnic Disparities in COVID-19 Mortality
- Childcare Survey and Data Display
- Risk of Complications Conditional on COVID-19 Infection
- Travel Time to COVID Testing Sites in Connecticut
- Travel Time to COVID Testing Sites in the US
- Project Team
- Issues List
- Print Magazine PDFs
- Print Newsletter PDFs
- YSM Events Newsletter
- Social Media
- Patient Care
INFORMATION FOR
- Residents & Fellows
- Researchers
Topical Shows Promise in Treating Precancerous Cervical Condition
A phase II trial led by Yale Cancer Center researchers shows promise as a non-invasive treatment for individuals with cervical intraepithelial neoplasia .
Dr. Alesssandro Santin on the Phase II study in Clinical Cancer Research
Cervical cancer, often caused by persistent human papillomavirus (HPV) infections, remains a public health challenge worldwide despite falling diagnoses related to the success of the HPV vaccine in young adult women. More than 11,500 women in the U.S. are diagnosed with cervical cancer each year, and over 4,000 women die from it.
A randomized three-arm (compares three different groups) phase II trial led by Yale Cancer Center (YCC) researchers at Yale School of Medicine examined the efficacy of imiquimod suppositories — which contain a topical drug that stimulates an immune system response — alone and in combination with the 9-valent human papillomavirus (9vHPV) vaccine in patients with cervical intraepithelial neoplasia (CIN), grades 2 and 3. CIN is a precancerous condition in which an individual develops abnormal cells at the entrance of the uterus (the cervix). It’s often caused by HPV strains.
YCC researchers presented the study’s findings at the American Association for Cancer Research (AACR) Annual Meeting in San Diego, California, on April 9. The results were simultaneously published in the journal Clinical Cancer Research .
A new treatment could be welcomed by women. Surgery is the standard treatment option for patients with CIN2 and CIN3, which can cause reproductive health complications.
In this study, YCC researchers investigated the efficacy of noninvasive immunomodulatory agents and vaccine treatments for women with CIN2 and CIN3. Women with CIN1, in which abnormal cells are the least severe, typically have a regression rate of over 90% over time and do not usually need surgery.
“With CIN1, we don’t do surgery; we advise the patients to come back and see us in 6 to 12 months, so we can repeat the pap smear,” said Alessandro Santin, MD , senior author of the study, professor of obstetrics, gynecology & reproductive sciences at YSM, and co-chief of the section of gynecologic oncology at YCC. “For CIN2 it is different," said Santin. “Our study shows that women with CIN2 have very high regression rates taking imiquimod. With the rate so high, it shows they don’t need surgery and can instead take this topical treatment.”
In this study, researchers randomly grouped 133 patients with CIN 2 (77%) and CIN 3 (23%) into three cohorts. One was treated with imiquimod, another combined the use of imiquimod with the protective shield of the 9vHPV vaccine, and a third group was monitored through clinical surveillance, serving as the control.
The results were positive, well-exceeding regression (reduction of abnormal cells) rates of past retrospective studies for women with CIN2: Ninety-five percent of those treated with imiquimod alone saw their condition regress to levels typically seen with CIN1 (lowest severity) or better, compared to the 79% in the surveillance group. The addition of the 9vHPV vaccine to imiquimod treatment resulted in an 84% regression rate, suggesting that the medication and HPV vaccine may impact the success of each other.
“The imiquimod treatment was patient-friendly and easy to use, since it could be applied by the patient without requiring an office visit,” said Sangini Sheth, MD, MPH , first author of the study, YSM associate professor of obstetrics, gynecology & reproductive sciences, and director of the Colposcopy and Cervical Dysplasia Program, Gynecologic Specialties. “It was also well-tolerated by the study participants, who experienced minimal side effects.”
The trial's results provide evidence for noninvasive procedures to potentially replace surgery as the best strategy for managing CIN2 and possibly CIN3. Santin would like to see future studies that investigate imiquimod for cervical intraepithelial neoplasia include a higher percentage of patients with CIN3.
In addition to Santin and Sheth, Stefania Bellone , Michelle Greenman , Levent Mutlu , Blair McNamara , Shefali Pathy , Mitchell Clark , Masoud Azodi , Gary Altwerger , Vaagn Andikyan , Gloria Huang , Elena Ratner , Daniel J Kim , Akiko Iwasaki , Angelique Levi , Natalia Buza , Pei Hui , Sean Flaherty , and Peter Schwartz were Yale co-authors.
Featured in this article
- Alessandro Santin, MD Professor of Obstetrics, Gynecology, and Reproductive Sciences; Clinical Research Team Leader, Gynecologic Oncology, Yale Cancer Center; Co-Chief, Section of Gynecologic Oncology
- Sangini S Sheth, MD, MPH, FACOG Associate Professor, Obstetrics, Gynecology and Reproductive Sciences; Affiliated Faculty, Yale Institute for Global Health; Director of Diversity, Equity, & Inclusion (DEI), Obstetrics, Gynecology & Reproductive Sciences; Associate Chief, Gynecologic Specialties; Director of Colposcopy and Cervical Dysplasia, Gynecologic Specialties
- Elena Ratner, MD, MBA Professor of Obstetrics, Gynecology & Reproductive Sciences; Co-Chief, Section of Gynecologic Oncology
- Stefania Bellone, PhD Associate Research Scientist in Obstetrics, Gynecology, and Reproductive Sciences
- Michelle Greenman Clinical Associate
- Levent Mutlu, MD Instructor
- Blair Colette McNamara, MD Instructor
- Shefali Pathy, MD, MPH Assistant Professor of Obstetrics, Gynecology & Reproductive Sciences; Site Director, Women's Health Sargent Drive; Clerkship Director, Obstetrics, Gynecology & Reproductive Sciences
- Mitchell Clark, MD, MPH Assistant Professor of Obstetrics, Gynecology & Reproductive Sciences; Director, Gynecologic Oncology at Waterford; Assistant Program Director, Minimally Invasive Gynecological Surgery Program; Associate Director, Center for Precision Diagnosis of Trophoblastic Disease

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- v.101(1); 1964 Jul
CASE STUDIES IN OBSTETRICS AND GYNECOLOGY
Full text is available as a scanned copy of the original print version. Get a printable copy (PDF file) of the complete article (228K), or click on a page image below to browse page by page.
- Open access
- Published: 05 April 2024
The COVID-19 pandemic and OBGYN residency training: We have a problem and it’s not just masks
- Alexandria C. Kraus 1 ,
- Anthony Bui 2 ,
- Kimberly Malloy 1 ,
- Jessica Morse 3 &
- Omar M. Young 1
BMC Medical Education volume 24 , Article number: 377 ( 2024 ) Cite this article
214 Accesses
2 Altmetric
Metrics details
The COVID-19 pandemic has left no one untouched. Resident trainees have been driven to reconsider virtually every component of their daily lives. The purpose of this pilot study is to evaluate the impact of the COVID-19 pandemic on Obstetrics and Gynecology (OBGYN) residency training and education.
A cross-sectional pilot study was conducted between 2/2022 and 5/2022. A survey was created and distributed to OBGYN residents. The survey queried the effects of the pandemic on OBGYN residents’ procedure skills training and mental health.
A total of 95 OBGYN residents across programs affiliated with each American College of Obstetricians and Gynecologists (ACOG) district participated in the survey. Among them, just over half ( n = 52, 55%) self-identified as under-represented minorities. A significant majority, 80% ( n = 81), felt their gynecological training was inadequate, with 70% of fourth-year residents expressing a lack of confidence in their ability to independently practice gynecology after graduation. This lack of confidence among fourth-year residents suggests a notable disparity in readiness for independent gynecological practice, linked to meeting ACGME requirements before completing their residency ( p = 0.013). Among the residents who reported a negative impact of the pandemic on their mental health ( n = 76, 80%), about 40% ( n = 31) had contemplated self-harm or knew a colleague who considered or attempted suicide ( p < 0.001). This issue was especially pronounced in residents experiencing burnout ( n = 44, 46%), as nearly half ( n = 19, 43%) reported suicidal thoughts or knew someone in their program who had such thoughts or engaged in self-harm ( p = 0.048).
Conclusions
Residents expressed concerns about reduced hands-on gynecological training and doubts about their readiness for independent practice post-residency, highlighting the need for enhanced support through mentorship and revised training curriculums. Additionally, despite the availability of mental health resources to address pandemic-induced burnout, their underuse suggests a need for more accessible time for residents to use at their discretion and flexible training schedules that encourage mental health support resource utilization.
Peer Review reports
Introduction
The disease known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first described in China in December of 2019 [ 1 ], and in March of 2020, the World Health Organization (WHO) declared the SARS-CoV-2 (i.e., COVID-19) outbreak a pandemic [ 2 ]. The disease has left no one untouched. The healthcare industry specifically has been overwhelmed by the effect of COVID-19 on resources with providers driven to reconsider virtually every component of their daily lives and practice. To sustain adequate hospital resources, elective surgical procedures were cancelled, and clinical volumes were dramatically reduced. Telemedicine was utilized to provide a significant portion of outpatient healthcare and inpatient care teams were condensed.
Resident schedules, in particular, were modified to provide a workforce where necessary and educational curricula transitioned toward virtual platforms in attempts to avoid exposures and to enforce social distancing [ 3 ]. While virtual solutions were implemented to counteract missed in-person pedagogic didactics and conferences, there were no immediate substitutes for the significant reduction of hands-on clinical and surgical experiences during this period. Additionally, visitor restrictions impacted the development of resident communication skills and emotional intelligence. Infected residents often required long absences, which resulted in re-assignments of remaining residents and trickle-down effects on overall residency training and education. Nonetheless, limited studies have been published on the impact of COVID-19 on residency training [ 4 , 5 , 6 ], and specifically, in the field obstetrics and gynecology (OBGYN) training [ 7 , 8 , 9 , 10 ]. Therefore, the purpose of this pilot study is to examine the impact of the COVID-19 pandemic on OBGYN residency training and education.
A nationwide, cross-sectional pilot study was conducted between February 2022 and May 2022. An anonymous survey was created using Qualtrics XM, (an online, secure survey platform), and OBGYN residents across the United States were invited to participate. The survey was preceded by a statement (1) explaining the purpose of the survey, (2) clarifying that the data would be de-identified before analysis and (3) delineating that program leadership would not have access to the responses. There were no incentives to participate. The study was reviewed and determined to be exempt by the Institutional Review Board (IRB #22–0136). A link to the survey was e-mailed to OBGYN program directors and program managers with a request that it be forwarded to all the residents in their program. The emails of the program directors and program managers were obtained from the Association of Professors of Gynecology and Obstetrics (APGO) website [ 11 ]. Reminder emails to encourage participation were distributed every four weeks for a period of three months. Recruitment posts were placed on social media as well. Responses were captured anonymously to maintain confidentiality.
All OBGYN residents in the United States were eligible to participate [ 12 ]; however, it is unclear how many residents received access to the survey, as there was limited verification from residency program leadership confirming distribution. In addition, multiple emails to both program directors and program managers were returned as invalid, further suggesting that many residency programs did not receive access to the survey at all. As such, it is difficult to report an accurate response rate.
The 28-question survey was developed after a comprehensive examination of the contemporary literature and following a review by local content experts to improve overall quality as well as to ensure content validity among assessed domains. Attention was paid to the Accreditation Council for Graduate Medical Education (ACGME) core competencies [ 13 ], and in particular, patient care, procedure skills, and medical knowledge, when devising and organizing the survey questions. We were also acutely aware of the potential impact of the pandemic on personal attitudes and a portion of the survey was dedicated to inquiring about resident well-being and burnout.
Demographic and program information was collected and included the following: clinical postgraduate year (PGY), age, race/ethnicity, gender, and residency program location (based on The American College of Obstetricians and Gynecologist (ACOG) District). With respect to patient care and procedural skills, the survey specifically queried residents about modifications to their schedules, duty hours, operative volume (major and minor surgical procedures), clinical duties, and availability and use of personal protective equipment (PPE). Residents were also asked if these changes affected their graduation requirements and overall preparedness for their postgraduate careers. When considering the impact of COVID-19 on residents’ medical knowledge, we asked about changes to educational curricula and their impact on rotation evaluations and CREOG scores. Finally, we attempted to determine the psychological effect of the pandemic on resident well-being and asked about resources provided by residency programs to combat potential burnout. The full survey is available for review in Appendix 1.
Descriptive analysis was used to summarize the data. Statistical analysis was performed using χ 2 test or Fisher’s exact test as appropriate for categorical data and Wilcoxon rank sum test for continuous data. P values of < 0.05 were considered significant. All analyses were performed using multiprocessor Stata 17.0 (StataCorp LP, College Station, Texas).
One hundred thirty-five OBGYN residents initiated the survey; however, only 95 residents completed the survey in its entirety. All respondents were vaccinated and trained at programs representing each ACOG District. The respondent demographics are detailed in Table 1 . The majority of participants ( n = 61, 64.2%) were senior OBGYN residents (i.e., PGY3 or PGY4). Eighteen (18.9%) residents self-identified as PGY1s and 16 (16.8%) as PGY2s. Most were between 25 and 34 years of age ( n = 88, 92.6%) and more than half of the residents ( n = 52, 54.7%) self-identified as under-represented minorities (i.e., Black or LatinX). Thirty-two (33.7%) residents had been personally infected by COVID-19, and 38 (40%) had immediate household contacts who contracted COVID-19.
Eighty-two (86.3%) residents felt that their residency training had been adversely affected by COVID-19, and 70 (73.7%) had an interruption in their regularly scheduled residency training; however, over 75% ( n = 76) of resident participants believed that their CREOG scores and rotational evaluations were unchanged during the pandemic. With respect to their procedural training, most residents ( n = 75, 78.9%) did not think their obstetrical training had been deleteriously affected, while over 80% ( n = 81) of residents felt that their gynecological training had suffered. Moreover, over half ( n = 55, 57.9%) of respondents trained at institutions where restrictions were placed on gynecological procedures for greater than eight weeks. The approximate numbers of gynecological procedures performed by residents by clinical postgraduate year are illustrated in Table 2 . OBGYN minimum numbers (which represent what the ACGME Review Committee [ 14 ] believes to be an acceptable minimal experience for OBGYN residents) are listed as well for reference. Of note, self-reported obstetrical numbers by clinical postgraduate year are described in Supplemental Table 1 for additional review.
As expected, there were significant differences in approximate gynecological numbers by clinical postgraduate year, with increasing numbers from PGY1 to PGY4 ( p < 0.001). Notably, the median procedure numbers among 4th-year residents were all above the minimum ACGME requirements; however, the lower quartile of self-reported gynecological numbers for vaginal hysterectomies (15 (10.75–16.75)) and incontinence and pelvic floor procedures (25.5 (20.5–30)) were below the minimum ACGME requirements, indicating that the lower quartile of PGY4 respondents were likely not meeting these gynecological procedure minimums.
When asked about reaching their ACGME minimums, over a third ( n = 40, 42.1%) of respondents were unsure if they would be able to achieve these minimum requirements by graduation. Moreover, almost 65% ( n = 60) of residents stated that they were not confident they could practice gynecology independently upon graduation. In contrast, approximately 87% ( n = 83) of OBGYN respondents believed they were poised to practice obstetrics autonomously following residency.
Responses from 4th-year residents to these survey questions are specifically examined in Table 3 . When analyzing the responses of those PGY4 respondents who were worried they would not reach their ACGME minimums by graduation, a significant proportion of residents were not confident in their ability to practice gynecology independently following graduation. Namely, of the 27 4th-year OBGYN respondents, seven (26%) were not certain they would attain their ACGME minimums, and of those seven, over 70% ( n = 5) did not feel prepared for autonomous practice of gynecology following graduation. Of those PGY4 residents who thought they would attain their ACGME minimums ( n = 20, 74%), approximately 80% ( n = 4) felt assured about their self-directed performance of gynecologic procedures after residency. These findings illustrate that there is a significant difference in the proportion of 4th-year residents ready for independent practice in gynecology depending on their ability to meet their ACGME requirements by graduation from residency ( p = 0.013). This difference did not persist when investigating respondents’ confidence in independent post-graduation obstetrics practice and meeting ACGME minimum requirements ( p = 0.756).
A significant portion of the survey attempted to determine the psychological effect of the pandemic on resident well-being. When asked about the use of personal protective equipment (PPE) when caring for patients infected with COVID-19, 20% ( n = 15) of residents reported they did not have access to adequate PPE. Forty-five (47.3%) respondents reported violating the 80-hour per week duty requirement, and 15 residents (15.8%) reported having less than four days off per month on average during the pandemic. Over 45% ( n = 44) of OBGYN residents conveyed that the pandemic interfered with their ability to perform at work, and 80% ( n = 76) stated that COVID-19 had adversely influenced their mental health. Notably, 31 (32.6%) participants maintained that they had, or knew another OBGYN resident that had suicidal thoughts or had attempted self-harm or suicide.
Additional questions inquired about the support provided by residency programs and institutions to combat burnout. Over 70% of residents ( n = 67) considered their residency leadership supportive of their wellness and education during the pandemic. Moreover, 80 (84.2%) OBGYN respondents stated that their institution had mentalhealth resources available; however, only 28 (29.4%) of residents utilized such resources.
The data on residents’ perceptions of the pandemic’s impact on mental health and their ability to perform at work (a measure used to indicate burnout) is correlated with their views on residency support, suicidal thoughts, access to wellness resources, and utilization of mental health services, as presented in Table 4 . Of those residents ( n = 76) who communicated the negative influence of the epidemic on their mental health, approximately 40% ( n = 31) had thoughts of or knew a fellow OBGYN resident who had had thoughts of self-harm, or even potentially attempted suicide ( p < 0.001). This significant finding persisted among those residents who suffered from burnout ( n = 44) as almost half ( n = 19, 43.2%) of those residents reported suicidal thoughts or actions either themselves or among those within their residency program ( p = 0.048). In contrast, of those residents who affirmed that their mental health was unaffected by the pandemic ( n = 18), none communicated suicidal thoughts or attempted self-harm.
Our data demonstrates that COVID-19 has had a grave academic and psychologic impact on OBGYN residents across the country. Procedural training in gynecology was particularly impacted. Over 80% residents reported that their gynecological training had suffered and over half of respondents trained at institutions where restrictions were placed on gynecological procedures for greater than eight weeks. When asked about attaining their ACGME minimums, over a third of residents were unsure if they would be able to achieve these requirements in gynecology by graduation, and approximately two-thirds of respondents stated that they were not confident that they would be able practice gynecology independently following graduation from residency. When concentrating on graduating (i.e., 4th-year) resident responses, there was a significant difference in the proportion of residents reporting readiness for intendent practice in gynecology depending on their ability to meet their ACGME requirements by graduation from residency.
Resident mentalhealth was also negatively altered by the pandemic. Nearly half of OBGYN residents reported that the pandemic interfered with their ability to perform at work. While over two-thirds of residents stated that their institution had mentalhealth resources available, less than a third of residents utilized such resources. Most notably, almost a third of residents maintained that they had, or knew another OBGYN resident that had, suicidal thoughts or had attempted self-harm or suicide– emphasizing the profound psychological effect of the pandemic.
Our pilot study contributes to the emerging body of research on the effects of the COVID-19 pandemic on OBGYN residents [ 8 , 9 , 10 ]. It corroborates findings from Europe, where OBGYN residents experienced reduced surgical training and teaching, leading to concerns about the quality of patient care [ 15 ]. Work by Harzif et al., also complements this by examining the psychological impact (i.e., anxiety, depression, and psychological trauma) of the pandemic on Indonesian OBGYN residents [ 16 ]. Additionally, a cross-sectional survey by Winkle et al., delved into if residents’ self-reported experiences of burnout and other issues, such as depression, binge drinking, and drug use, vary according to their personal activities, including hobbies [ 17 ]. Further research suggested that resident-led wellness initiatives, like providing discretionary time and promoting social events, were the highest rated in supporting resident wellness [ 18 ]. Akin to our study findings, Wadell et al., found residents worried about the pandemic’s detrimental effects on their training, particularly among senior residents [ 19 ]. This anxiety is intensified by a national decrease in gynecologic surgeries and fellowship directors’ reports of new fellows’ unpreparedness for independent surgical practice [ 20 , 21 ].
Our pilot study has several strengths and is the first of its kind to examine the impact of COVID-19 on OBGYN trainees in the United States. Our survey was conducted nationally with representation from respondents training at centers in each of the ACOG districts at a time when the direct effects of the pandemic on training were either ongoing or still very fresh in respondents’ memories, minimizing the impact of recall bias. Furthermore, while small, more than half of the residents self-identified as underfrepresented minorities, indicative of a diverse respondent population. The findings in our pilot study are suggestive of associations that should be replicated in larger samples.
Nonetheless, our pilot study has limitations, namely our low overall response rate and potential for selection bias. It is unclear how many residents received access to the survey, as there was limited verification from residency program leadership confirming distribution. Significant differences between responders and non-responders could have been overlooked. Our use of a volunteer population may not be representative of the general OBGYN resident population, and it is possible that those residents who felt more strongly about their experiences were more likely to respond. Our pilot study was also not longitudinal and cannot be translated to assess long-term effects.
The COVID-19 pandemic has left virtually no one unharmed. Resident trainees, in particular, have been forced to reexamine their daily lives and practice. OBGYN residents in the United States reported concerns about their abilities for autonomous gynecological practice upon completion of residency, lending us the opportunity to provide increased support to new graduates through both formal and informal mentorship. Other potential solutions include both institutional and national working groups on gynecological procedural minimums and considerations of more flexible curriculums such as tracking. Efforts could also be made to develop surgical simulation training programs so trainees can maximize their surgical learning in the operating room. Respondents also conveyed that the pandemic deleteriously affected their mentalhealth, and while support was provided by their residency programs with resources available at their institutions to combat burnout, few residents utilized such resources. A promising solution includes the broader adoption of institution-based wellness programs and increased flexibility and time-off within clinical training to make use of institutional resources. Further large-scale investigations verifying these findings are critical.
Data availability
Data and materials can be obtained from the corresponding author upon reasonable request.
Guidance for maternal medicine services in the coronavirus (COVID-19). pandemic. https://www.rcog.org.uk/globalassets/documents/guidelines/2020-07-10-guidance-for-maternal-medicine.pdf . Published July 10, 2020. Accessed September 21, 2021.
WHO Director-General’s. opening remarks at the media briefing on COVID-19–11 March 2020.Who.int. https://www.who.int/director-general/speech/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19----11-march-2020 . Published 2021. Accessed January 17, 2022.
Who coronavirus (COVID-19) dashboard. World Health Organization. https://covid19.who.int/ . Accessed January 17, 2022.
Accreditation Council for Graduate Medical Education. ACGME Response to Coronavirus (COVID19). Last Updated, March 18, 2020. https://acgme.org/Newsroom/NewsroomDetails/ArticleID/10111/ACGME-Response-to-the-Coronavirus-COVID-19 . Accessed March 20, 2020.
Zingaretti N, Negrini C, Tel F. The impact of COVID-19 on plastic surgery residency training. Aesth Plast Surg. 2020;44:1381–5. https://doi.org/10.1007/s00266-020-01789-w . https://doi-org.libproxy.lib.unc.edu/ .
Article Google Scholar
Huntley RE, Ludwig DC, Dillon JK. Early effects of covid-19 on oral and maxillofacial surgery residency training—results from a national survey. J Oral Maxillofac Surg. 2020;78(8):1257–67. https://doi.org/10.1016/j.joms.2020.05.026 .
Aziz H, James T, Remulla D, et al. Effect of covid-19 on surgical training across the United States: a national survey of general surgery residents. J Surg Educ. 2021;78(2):431–9. https://doi.org/10.1016/j.jsurg.2020.07.037 .
Bitonti G, Palumbo AR, Gallo C, et al. Being an obstetrics and gynaecology resident during the covid-19: impact of the pandemic on the residency training program. Eur J Obstet Gynecol Reproductive Biology. 2020;253:48–51. https://doi.org/10.1016/j.ejogrb.2020.07 .
Yalçın Bahat P, Aldıkaçtıoğlu Talmaç M, Bestel A, Topbas Selcuki NF, Karadeniz O, Polat I. Evaluating the effects of the COVID-19 pandemic on the physical and mental well-being of obstetricians and gynecologists in Turkey. Int J Gynaecol Obstet. 2020;151(1):67–73. https://doi.org/10.1002/ijgo.13287 .
Gothwal M, Singh P, Sharma C, Yadav G, Gupta MK. Impact of COVID-19 pandemic on obstetrics and gynecology residency training program in India: a national online survey. J Obstet Gynaecol Res. 2022;48(7):1955–60. https://doi.org/10.1111/jog.15291 .
Residency APGO. (2021, April 8). Retrieved December 29, 2022, from https://tools.apgo.org/residency-directory/ .
Table B3: Number of active residents, by type of medical school, GME specialty, and sex. AAMC. https://www.aamc.org/data-reports/students-residents/data/table-b3-number-active-residents-type-medical-school-gme-specialty-and-sex . Accessed March 26, 2023.
Milestones guidebook for residents and fellows - ACGME. https://www.acgme.org/globalassets/PDFs/Milestones/MilestonesGuidebookforResidentsFellows.pdf . Accessed November 28, 2022.
Case log information: Obstetrics and gynecology - ACGME. https://www.acgme.org/globalassets/pfassets/programresources/obgyncaseloginfo.pdf . Accessed December 12, 2022.
Boekhorst F, Khattak H, Topcu EG, Horala A, Goncalves Henriques M. The influence of the COVID-19 outbreak on European trainees in obstetrics and gynaecology: A survey of the impact on training and trainee. Eur J Obstet Gynecol Reprod Biol. 2021;261:52–58. https://doi.org/10.1016/j.ejogrb.2021.04.005 .
Harzif AK, Lukman DDS, Maidarti M, et al. Social factors influence on anxiety, depression level and psychological trauma of obstetrics and gynecology residents during COVID-19 pandemic. Heliyon. 2022;8(12):e12271. https://doi.org/10.1016/j.heliyon.2022.e12271 .
Winkel AF, Woodland MB, Nguyen AT, Morgan HK. Associations Between Residents’ Personal Behaviors and Wellness: A National Survey of Obstetrics and Gynecology Residents. J Surg Educ. 2020;77(1):40–44. https://doi.org/10.1016/j.jsurg.2019.08.014 .
Seeland GR, Williams BM, Yadav M, et al. Implementation and Evaluation of a Comprehensive Resident Wellness Curriculum During the COVID-19 Pandemic. J Surg Educ. Published online December 21, 2023. https://doi.org/10.1016/j.jsurg.2023.11.014 .
Wadell M, Ortqvist AK, Linden K, et al. Challenges imposed by the COVID-19 pandemic on the Obstetrics and Gynecology residency program: a mixed-methods Swedish survey in the COPE Staff cohort study. BMC Med Educ. 2022;22(1):602. Published 2022 Aug 5. https://doi.org/10.1186/s12909-022-03631-0 .
Wright JD, Herzog TJ, Tsui J, et al. Nationwide trends in the performance of inpatient hysterectomy in the United States. Obstet Gynecol. 2013;122(2 Pt 1):233–241. https://doi.org/10.1097/AOG.0b013e318299a6cf .
Guntupalli SR, Doo DW, Guy M, et al. Preparedness of Obstetrics and Gynecology Residents for Fellowship Training. Obstet Gynecol. 2015;126(3):559–568. https://doi.org/10.1097/AOG.0000000000000999 .
Download references
Acknowledgements
We would like to thank all the residents who participated in our study.
No significant sources of funding.
Author information
Authors and affiliations.
Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, University of North Carolina at Chapel Hill, 3010 Old Clinic Building, Chapel Hill, NC, 27599, USA
Alexandria C. Kraus, Kimberly Malloy & Omar M. Young
Department of Obstetrics and Gynecology, University of North Carolina at Chapel Hill, Chapel Hill, USA
Anthony Bui
Division of Family Planning, Department of Obstetrics and Gynecology, University of North Carolina at Chapel Hill, Chapel Hill, USA
Jessica Morse
You can also search for this author in PubMed Google Scholar
Contributions
A.K. wrote the main manuscript text. A.B. was responsible for the statistical analysis. All authors reviewed the manuscript.
Corresponding author
Correspondence to Alexandria C. Kraus .
Ethics declarations
Ethics approval and consent to participate.
The study was performed in accordance with the Declaration of Helsinki and approved by The University of North Carolina at Chapel Hill IRB (#22–0136). Participation was voluntary, anonymized, and performed under a waiver of informed consent following review by The University of North Carolina at Chapel Hill IRB.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary material 2, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Kraus, A.C., Bui, A., Malloy, K. et al. The COVID-19 pandemic and OBGYN residency training: We have a problem and it’s not just masks. BMC Med Educ 24 , 377 (2024). https://doi.org/10.1186/s12909-024-05364-8
Download citation
Received : 18 June 2023
Accepted : 28 March 2024
Published : 05 April 2024
DOI : https://doi.org/10.1186/s12909-024-05364-8
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Obstetrics and gynecology
- Surgical training
- Mental health
- United States
BMC Medical Education
ISSN: 1472-6920
- Submission enquiries: [email protected]
- General enquiries: [email protected]
Obstetrics and Gynecology
- Mayo Clinic pilot study pinpoints resectable high-grade serous ovarian cancer
April 10, 2024

In a pilot study, Amanika Kumar, M.D. , a gynecologic oncologist at Mayo Clinic in Minnesota, and colleagues found that CT plus tumor molecular subtyping of patients with advanced-stage high-grade serous ovarian cancer (HGSOC) provides crucial presurgical information. These two tests furnish results indicating which patients have low likelihood of successful disease resection and require significantly complex surgery. Gynecologic Oncology published the pilot study's findings in 2022.
Dr. Kumar and colleagues intend the CT plus molecular subtyping for use in tandem with other clinical factors to improve resectability prediction. Knowing with greater certainty whether disease resection is likely to be successful increases informed decision-making for the surgeon and the patient.
Significance of study results
Inspiring this study is what Dr. Kumar calls "an obsession with residual disease" of her gynecologic oncology team treating patients with HGSOC. This obsession developed because any postsurgical residual disease beyond 1 cm signifies that the resection will not improve the patient's situation, says Dr. Kumar. Resection to no gross residual disease is really the goal.
"This is why high-quality surgery is imperative for advanced ovarian cancer," she says.
Having the same outlook before and after surgery would be a significant setback for a patient who has HGSOC and the surgeon, as this operation is complex and involves:
- Surgery lasting 6 to 8 hours.
- Substantial blood loss.
- Work in all four abdominal quadrants.
- Significant risk.
Dr. Kumar notes that although the risk of death is low in HGSOC resection, risk of major complications is 10% to 15%.
"These are huge surgeries with a lot of costs," says Dr. Kumar. "We proceed with them, however, because this surgery, if resulting in no gross residual disease, is life-prolonging for a serious cancer problem. There's a big survival difference depending on amount of postsurgical residual disease."
At Mayo Clinic, this desire to achieve no gross residual disease has led to expansion of surgical education and services offered.
If a patient undergoes chemotherapy alone without surgery for HGSOC, however, Dr. Kumar indicates outcomes are "pretty bad — years of survival different than with high-quality disease resection."
Yet Dr. Kumar says she has seen patients opt out of surgery if longevity is not a goal, and she respects this position.
A CT scan can accurately predict resectability in about 60% of people who undergo surgery, which is good but not great, she says. With the addition of molecular subtyping as performed in this pilot study, however, the gynecologic oncologist also can learn the following critical information about a patient's disease, which conveys potential resection success:
- Tumor type.
- Tumor gene expression.
- Categorization by The Cancer Genome Atlas.
"Using more and novel information really personalizes patient care, particularly surgery," says Dr. Kumar.
Dr. Kumar and research colleagues call for a confirmatory study of this combination of resectability decision-making factors. They also believe that AI tools hold resectability prediction potential to help more patients. Currently, she and her colleagues are not using the molecular profiling and CT combination clinically to determine resectability due to the need for a prospective study to further validate this approach. Until then, they will continue determining resectability through physical exam, medical history and symptom assessment, and review of imaging results.
HGSOC treatment
For anyone diagnosed with ovarian cancer, high-quality surgery is critical for optimal outcome, says Dr. Kumar. Typically, patients diagnosed with HGSOC require chemotherapy and surgery. Conventional wisdom in the field indicates that the order of these treatments does not matter. However, Dr. Kumar and colleagues propose that upfront surgery produces the best outcomes if meaningful surgery leaves the patient without gross residual tumor.
A significant HGSOC surgical challenge this study attempted to rectify is the potential for the surgeon to discover, once opening the patient in the OR, that meaningful disease resection is impossible. This potential makes novel resectability prediction methods desirable.
The nature of HGSOC
Many know ovarian cancer as a silent killer with virtually no detectable symptoms. Eventually, 70% of patients diagnosed with ovarian cancer develop advanced disease spreading throughout the abdomen and sometimes the thorax, indicating poor prognosis, says Dr. Kumar.
Despite this prognosis, however, she indicates that highly effective treatment that can achieve remission is now available to help these patients.
"We are known for our advanced ovarian cancer treatment at Mayo Clinic and are constantly trying to push the edge. We want patients to see us in critical situations where we can make an impact, and we believe we can offer improved oncologic and surgical outcomes." — Amanika Kumar, M.D.
Referral of patients with HGSOC
For surgeons uncertain about performing HGSOC surgery resulting in less than 1 cm of gross residual disease, Dr. Kumar invites Mayo Clinic referrals. She notes that Mayo Clinic gynecologic oncologists prioritize innovative, multidisciplinary and team-based care.
Dr. Kumar also mentions that there is now good evidence — such as a 2016 publication by Cowan and colleagues in Annals of Surgical Oncology — that patients who have surgery with a gynecologic oncologist at a high-volume center have better outcomes compared with those who do not receive this type of care.
Other factors she says are critical for successful HGSOC care include anesthesia support and involvement of capable radiologists. These factors characterize Mayo Clinic's care for people with this complex disease.
"We are known for our advanced ovarian cancer treatment at Mayo Clinic and are constantly trying to push the edge," she says. "We want patients to see us in critical situations where we can make an impact, and we believe we can offer improved oncologic and surgical outcomes. Most patients we operate on with HGSOC go back to work after surgical recovery, if not retired, and activities that give them joy — living a life that they value."
For more information
Kumar A, et al. Into the future: A pilot study combining imaging with molecular profiling to predict resectability in ovarian cancer . Gynecologic Oncology. 166;2022:508.
The Cancer Genome Atlas (TGCA) . National Cancer Institute Center for Cancer Genomics.
Cowan RA, et al. Is it time to centralize ovarian cancer are in the United States? Annals of Surgical Oncology. 2016;23:989.
Refer a patient to Mayo Clinic.
Receive Mayo Clinic news in your inbox.
Related content.

- Medical Professionals
Your gift holds great power – donate today!
Make your tax-deductible gift and be a part of the cutting-edge research and care that's changing medicine.
COMMENTS
Case Study: Obstetrics and Gynecology. Embolization to Treat Uterine Fibroids with Bleeding and Severe Anemia. A 45-year old female Jehovah's Witness patient with a history of uterine fibroids and severe menorrhagia presented with shortness of breath, fatigue and weakness. She also had a history of deep venous thrombosis (DVT) and pulmonary ...
Ankit Gupta, Chandrakala Channappa, Mohamed Abdelkhalek Ramadan Ibrahim Elsheikh, Manjula Annappa. 2 April 2024. Aggressive precursor B cell ALL of cervix with obstructive uropathy. Anupama Bahadur, Rajlaxmi Mundhra, Poonam Gill, Ashok Singh. 2 April 2024. Submucous leiomyoma: an uncommon cause of heavy menstrual bleeding in early adolescence.
Maternal outcomes in pregnancies affected by varicella zoster virus infections: population-based study on 7.7million pregnancy admissions. J Obstet Gynaecol Res 2015;41:62-68. Crossref
Case Reports in Obstetrics and Gynecology publishes case reports and case series related to obstetrics, maternal-fetal medicine, gynecology, gynecologic oncology, uro-gynecology, reproductive medicine, infertility, and reproductive endocrinology. ... This study reports a case of uterine liposarcoma together with a literature review. At 52 years ...
1. Obstetrics-Case studies. 2. Gynecology-Case studies. 3. Women-Health and hygiene. L Howat, Pant II. Title. (Series; Clinical cases in emergency medicine). 618 Published in Australia by M~Graw~Hm Australia Pty Ltd Level 2, 82 Waterloo Road, North Ryde NSW 2113 Publishing Manager: Jo Munnelly Acquisitions Editor: Nicole Mech~n
Read this chapter of Clinical Cases in Obstetrics, Gynaecology and Women's Health, 3rd Edition online now, exclusively on AccessWorldMed. ... Featuring world-leading textbooks, case-based learning, and a variety of study tools, AccessWorldMed offers a diverse range of resources with rich real-world examples that are aligned to local curricula ...
is uncertain and the vast majority are benign. In this specific case all the differential diag-noses are effectively excluded by the history and examination. 100 Cases in Obstetrics and Gynaecology 2 • Cervical malignancy • Cervical ectropion • Endocervical polyp • Atrophic vaginitis • Pregnancy • Irregular bleeding related to the ...
Labor and Delivery. The Editors of AJOG have worked with an international group of experts to create a comprehensive collection of information to optimize care and advance safe childbirth for women everywhere. Labor and Delivery Part 1. Labor and Delivery Part 2. Original Research Gynecology.
The October 2023 issue of Obstetrics & Gynecology will be dedicated exclusively to issues of racism and reproductive health and tangible steps that we can take to pave the path to health equity. The call for papers is available at https://bit.ly/3wKXvHg . On October 25, we hosted a webinar to engage potential authors and reviewers, and to ...
Case Rep Obstet Gynecol; Case Reports in Obstetrics and Gynecology Vols. 2011 to 2024; 2011 to 2024 ... 2017: v.2018 2018: v.2019 2019: v.2020 2020: 2011 to 2015: v.2011 2011: v.2012 2012: v.2013 2013: v.2014 2014: v.2015 2015: Articles from Case Reports in Obstetrics and Gynecology are provided here courtesy of Hindawi Limited. Follow NCBI ...
Uterine torsion is rare in pregnancy and the cause in most cases is unknown. It is associated with fetal compromise, with perinatal mortality reported to be around 12%. Our case describes an acute torsion, presenting in pregnancy with severe abdominal pain and vomiting with a viable 32-week gestation. Emergency caesarean section was performed ...
As large studies are lacking, figures defining overall prognosis are variable and based on small case-series. ... cardiomyopathy or pre-eclampsia, with or without sepsis. This case emphasises the importance of close liaison between obstetrics and ICU services, as advocated by recent Royal College meetings, and hopefully reminds others of the ...
Ultrasound in Obstetrics & Gynecology (UOG), the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG), is the leading international peer-reviewed journal in the field.UOG features the latest, most clinically relevant research, including guidelines, consensus statements, expert commentaries, original articles and systematic reviews.
16.1 Case-based discussion questions. 1. Abdominal pain, bleeding, and rape. An 18-year-old attends the emergency department with abdominal pain and vaginal bleeding. Her last period was 1 week prior and she has not had intercourse since then.
In this ethical approach, care represents the fundamental orientation of obstetrics and gynecology as well as much of medicine and health care, and it indicates the direction and rationale of the relationship between professionals and those who seek their care. An ethic of care also joins case-based approaches in focusing on particular contexts ...
Abstract . BackgroundTo study the course of pancreatitis in pregnant women and demonstrate that early diagnosis and conservative management leads to good maternal and perinatal outcome.. Methods:This article is a retrospective case series study.Six patients with acute pancreatitis during pregnancy were seen in a tertiary referral based obstetric practice at our department in the last 5 years.
Obstetrics & Gynecology: June 9, 2022 - Volume - Issue - 10.1097/AOG.0000000000004839. doi: 10.1097/AOG.0000000000004839. Open. PAP. Metrics. Abstract. In Brief. As restrictions on abortion increase nationwide, it is critical to ensure ongoing access to abortion care throughout pregnancy. People may seek abortions later in pregnancy as a result ...
Since the 1916-27 epidemic, only sporadic cases have been described. Pathological studies have revealed encephalitis of the midbrain and basal ganglia, with lymphocyte (predominantly plasma cell) infiltration. ... Case Files Obstetrics and Gynecology 5 + obstetrics. 2016 • 619 Pages • 18.06 MB. Physiotherapy in Obstetrics and Gynaecology ...
current issue. current issue; browse recently published; browse full issue index; learning/cme
Study design and findings. In this case-control study, investigators divided women into three groups: 22 women who had fetal surgery at 22 to 28 weeks' gestation, 13 women with an indication for fetal surgery who did not have prenatal intervention, and 36 gestational age-matched controls.
Case-control studies begin at the end. Two groups of patients, those with disease (cases) and those without (controls), are compared to determine the degree of exposure to a presumed risk factor. ... 1 Department of Obstetrics and Gynecology, Women & Infants' Hospital, Brown University School of Medicine, Providence, Rhode Island. PMID: 8008310
Study measures reflect self-reported responses by postpartum individuals 12 to 14 months after having a live birth. ... 3 Department of Obstetrics and Gynecology, NewYork-Presbyterian/Columbia University Medical ... we conducted complete-case analysis. We conducted statistical tests using 2-sided tests and a significance level of P < .05 ...
Objectives The purpose of this study is to show the feasibility and surgical outcome of vNOTES retroperitoneal dissection and isolation of sentinel lymph nodes in overweight and obese patients with endometrial cancer. Materials and methods Four patients had undergone pelvic lymphadenectomy with a sentinel lymph node. Three patients were overweight, and one was obese with a BMI of 34.6 kg/m2 ...
Case Maps. COVID-19 in Connecticut Schools. Connecticut Towns COVID-19 Impact Dashboard. ... senior author of the study, professor of obstetrics, gynecology & reproductive sciences at YSM, and co-chief of the section of gynecologic oncology at YCC. "For CIN2 it is different. "But our study shows that women with CIN2 have very high ...
CASE STUDIES IN OBSTETRICS AND GYNECOLOGY - PMC. Journal List. Calif Med. v.101 (1); 1964 Jul. PMC1515571. As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not imply endorsement of, or agreement with, the contents by NLM or the National Institutes of Health.
The COVID-19 pandemic has left no one untouched. Resident trainees have been driven to reconsider virtually every component of their daily lives. The purpose of this pilot study is to evaluate the impact of the COVID-19 pandemic on Obstetrics and Gynecology (OBGYN) residency training and education. A cross-sectional pilot study was conducted between 2/2022 and 5/2022.
Case study of obstetric and gynaecology. My patient Madam Suzanna 29years old gravida 4 para 2+1 electively admitted at 32 weeks of period of amenorrhea for expectant management of twin pregnancy with asymptomatic placenta previa type II posterior. Currently patient is well and has no complain of pervaginal bleeding and fetal movement was good.
In a pilot study, Amanika Kumar, M.D., a gynecologic oncologist at Mayo Clinic in Minnesota, and colleagues found that CT plus tumor molecular subtyping of patients with advanced-stage high-grade serous ovarian cancer (HGSOC) provides crucial presurgical information.These two tests furnish results indicating which patients have low likelihood of successful disease resection and require ...
In many medical schools, students are exposed to obstetrics for 2 weeks during the third-year obstetrics and gynecology clerkship. Hence, the purpose of this study was to evaluate the effectiveness of a curriculum combining online obstetric modules and a normal spontaneous vaginal delivery (NSVD) simulation on medical student knowledge and comfort pertaining to obstetrics at the start of the ...
Maternal obstetric outcomes for the study and control groups are presented in Table 2.The composite adverse maternal outcome was significantly higher among those who underwent IOL (23.1% vs 9.8%, P < 0.01).Women who had an IOL had a longer duration of both the first and second stages of labor, higher rates of intrapartum CD, perineal tear grade 3/4, PPH, hemoglobin drop >4 g/dL, blood product ...