- Technical Help
- CE/CME Help
- Billing Help
- Sales Inquiries

Qualitative Data Analysis
This course provides an applied approach to qualitative data analysis through the lens of multiple methods and methodologies.
About this Course
The analysis of qualitative research data is a fundamental yet multifaceted process that requires careful attention to the unique qualities of qualitative research design. This course provides an applied, phenomenological approach to qualitative data analysis. It is designed for an interdisciplinary audience with examples taken from the nonprofit, commercial, and government sectors in the health and social sciences.
Undergraduate/graduate students, research staff, and IRB members in particular may find this course meaningful as an introduction to qualitative research methods.
Course Preview:
Language Availability: English
Suggested Audiences: Faculty, IRB Chairs, IRB Members, Research Staff, Undergraduate and Graduate Students
Organizational Subscription Price: $675 per year/per site for government and non-profit organizations; $750 per year/per site for for-profit organizations Independent Learner Price: $99 per person
Course Content
" role="button"> introduction to qualitative data analysis.
This module discusses the data analysis considerations shared by all qualitative methods and approaches this course covers. This includes the basic qualitative data analysis process and tools and the rigorous and ethical approaches to qualitative data analysis that apply across methods.
Recommended Use: Required ID (Language): 20971 (English) Author(s): Margaret R. Roller, MA - Roller Research
" role="button"> In-Depth Interview Method
This module begins with an overview of the basic in-depth interview method and its variations. This provides the foundation for the core discussions concerning the distinctive aspects of the in-depth interview method that affect qualitative data analysis, including quality and ethical considerations.
Recommended Use: Supplemental ID (Language): 20972 (English) Author(s): Margaret R. Roller, MA - Roller Research
" role="button"> Focus Group Discussion Method
To provide a basis for the core discussions, this module begins with an overview of the fundamentals of the focus group method and its variations. This provides an understanding of the distinctive aspects of the focus group method that affect qualitative data analysis, including quality and ethical considerations.
Recommended Use: Supplemental ID (Language): 20973 (English) Author(s): Margaret R. Roller, MA - Roller Research
" role="button"> Ethnography
Understanding the ethnographic approach and its variations is important to the discussion of data analysis. For this reason, the module begins with an overview of ethnographic research and the distinctive aspects of ethnography that affect qualitative data analysis, including quality and ethical considerations.
Recommended Use: Supplemental ID (Language): 20974 (English) Author(s): Margaret R. Roller, MA - Roller Research
" role="button"> Narrative Research
This module provides an overview of narrative research and its variations. It provides an overview of narrative research, which serves as a foundation for the core discussions concerning the distinctive aspects of the narrative research approach that affect qualitative data analysis. The module concludes with a discussion of quality and ethical considerations.
Recommended Use: Supplemental ID (Language): 20975 (English) Author(s): Margaret R. Roller, MA - Roller Research
" role="button"> Case Study Research
Case study research and its variations are examined at the start of this module. Then, distinctive aspects of case study research that affect qualitative data analysis are explored, including quality and ethical considerations.
Recommended Use: Supplemental ID (Language): 20976 (English) Author(s): Margaret R. Roller, MA - Roller Research
" role="button"> Qualitative Content Analysis Method
This module reviews the basic Qualitative Content Analysis (QCA) method and its variations. It also discusses the distinctive aspects of the QCA method that affect qualitative data analysis and the quality and ethical considerations that QCA presents.
Recommended Use: Supplemental ID (Language): 20977 (English) Author(s): Margaret R. Roller, MA - Roller Research
Who should take the Qualitative Data Analysis course?
The suggested audience includes students, faculty, and staff that want to learn more about the basics of qualitative data analysis and one or more of the discussed methods.
How long does it take to complete the Qualitative Data Analysis course?
This course consists of one required module and six supplemental modules. All learners should complete module 1 and then complete the supplemental modules as needed (20-30 minutes each).
" role="button"> Why should an organization subscribe to this course?
Organizational subscriptions provide access to the organization's affiliated members. This allows organizations to train individuals across the organization on how to properly conduct qualitative data analysis.
" role="button"> What are the standard recommendations for learner groups?
This course is designed such that learners should complete the first module and then any following method modules as needed.
" role="button"> Is this course eligible for continuing medical education credits?
This course does not currently have CE/CME credits available.
Related Content
This course provides learners with an understanding of how to improve study design, collect and analyze data, and promote reproducible research.
Essentials of observational research protocol design and development.
Foundational course that orients and prepares learners to engage with the scholarly publication process in an informed way.
An in-depth review of the development and execution of protocols.
Privacy Overview
Cookies on this website
We use cookies to ensure that we give you the best experience on our website. If you click 'Accept all cookies' we'll assume that you are happy to receive all cookies and you won't see this message again. If you click 'Reject all non-essential cookies' only necessary cookies providing core functionality such as security, network management, and accessibility will be enabled. Click 'Find out more' for information on how to change your cookie settings.
- Study with us
- Short Courses in Qualitative Research Methods
- Introduction to Analysing Qualitative Data
Study with us:
- Introduction to Qualitative Research Methods
- Introduction to doing Qualitative Interviews
- Introduction to conversation analysis and health care encounters
- Learning with the book: an introduction to qualitative research methods for health research

This course will provide you with a good introduction to qualitative data analysis. Our expert tutors will support you to develop and practice your analysis skills using a combination of online lectures, group discussions, and practical online workshops.
This two-day online course introduces the principles and practice of qualitative data analysis, with emphasis on thematic analysis.
Over two days our approachable and research-active experts will show that analysis is achievable though an accessible step-by-step process, and will provide de-identified data for you to work with. Day one begins by looking at organising data (coding categorising and theme development); day two explores 'finding a story' and developing your analysis to translate to a research paper or thesis chapter.
We aim to support those who are planning to undertake or manage qualitative research using in-depth or semi-structured interviews or qualitative observational data, and support those who have already collected qualitative data which they are unsure how to analyse. The thematic analysis approach used is also applicable to other kinds of qualitative data including observation, diaries, and other text sources. While the course is aimed at the needs of health and care professionals, researchers, academics and postgraduate students, the skills developed here apply to many settings - please ask us if you are unsure whether Analysing Qualitative Data is the course for you.
COURSE DELIVERY
Please note that some of the teaching sessions for this online course will involve you participating in live, interactive Zoom sessions, which will fall between the hours of 09:00 and 17:00 UK time . We are very happy to welcome bookings wherever you are internationally, but please make sure that you are able to attend video calls between these hours.
The course will include:
- Expert-led lectures (a mixture of live and pre-recorded) on the principles of qualitative data analysis, with emphasis on thematic analysis
- Demonstrations and small group work to develop skills in coding and categorising qualitative data and in data interpretation
- Practical online exercises considering how to conduct and recognise 'good quality' qualitative analysis
- Expert feedback to support your learning and understanding
Learning outcomes
Learning Outcomes
By the end of the course participants will:
- Have an understanding of the principles of qualitative data analysis with emphasis on thematic analysis
- Have gained practical experience of coding, categorising, and conceptualising qualitative data or qualitative observational data using a thematic analysis approach
We provide:
- Access to the online learning platform (CANVAS)
- Online access to slides and materials
- De-identified data for you to work on whilst developing your skills
- Experienced, approachable tutors who are research-active
Online course
Date: 11-12 March 2024
Course details:
Course fee: £750 Duration: 2 days Total places: 24 Venue: Online Course
If you have any questions and queries please email us

“Fantastic teaching, great content, personal insight / experiences, putting it into practice and great to meet so many other people involved in qual research... Excellent course!”
“It has been a real privilege to attend a course led by such high quality, high calibre speakers – sharing the theory but intertwined with the reality of their own experiences and interests and passions.”
"A highlight was realising how far I’d come and how much I’d learned! Feeling inspired to try out what I’ve learned, thank you”
COURSE TUTORS

Lisa Hinton

Catherine Pope

Sue Ziebland
and expert tutors from the Medical Sociology & Health Experiences Research Group team
Oxford Qualitative Courses
This highly-regarded programme is delivered in online and face to face formats to suit a range of learners. We use a mixture of lectures and small group work, delivered by our team of qualitative researchers from the University of Oxford’s Medical Sociology and Health Experiences Research Group . Our group has run these successful courses for almost twenty years alongside active involvement in qualitative research on a variety of different topics, ranging from studies of personal experiences of health conditions and of healthcare practice, to evaluations of organisational change. Our group also includes qualitative methodologists at the forefront of developing qualitative methods including conversation analysis and evidence synthesis.
Findings from our group’s research on patient experiences, together with supported video, audio and text extracts, have been compiled to form the multi-award winning heathtalk.org website and its sister site socialcaretalk.org . Our portfolio of research and expertise informs current local, national and international healthcare policy and research.
The syllabuses of our qualitative courses draw on a wide range of expertise from within our research group, including the disciplinary areas of medical sociology, anthropology, and public policy.
Receive our bulletin:
Our courses are popular and often sell-out quickly. To receive a bulletin of upcoming course dates, please register here .
Got a question? Contact us:
Our friendly team are on-hand to answer your questions and queries.
Email: [email protected]
Make a Gift
Qualitative Research
The Odum Institute provides ongoing consulting services and short courses on qualitative research and related software. Qualitative research is a social scientific method for collecting textual, visual, or audio data.
Consultations & Guest Lectures
Consultations.
If you have questions regarding research design, data collection, strategies for analysis, and options for reporting findings , please contact Paul Mihas using the information provided below. Paul can also provide consultations on deductive, inductive, and abductive perspectives that inform qualitative research.
Paul can help you through any of the stages of your project, including the early stages of developing research questions and proposal writing, such as: Designing a study, data collection, analysis, developing research products .

Assistant Director of Qualitative and Mixed Methods Research
Guest lectures.
Time permitting, Paul is also available to give guest lectures on various qualitative research topics at classes and meetings. If you would like to schedule a guest lecture on a qualitative research topic, please contact Paul Mihas directly or visit our guest lecture page .
Back to top
Qualitative Research Traditions
- Generic qualitative
- Thematic qualitative research
- Phenomenology
- Ethnography
- Narrative Analysis
- Grounded Theory
Mixed Methods
Paul can also assist if you are conducting a study combining or connecting qualitative and quantitative data. Please visit our mixed methods page for more information.
Project Planning, Data Collection and Analysis
As part of a fee-based service , the Odum Institute offers project-based design and analysis using strategies customized for each project’s needs. These range from evaluation projects to multi-year research studies. Assistant Director Paul Mihas, with the assistance of graduate students, can help with:
- Research design
- Developing interview and focus group guides
- Conducting data collection
- Data analysis using specialized software
- Final reports
Dissertation & Master’s Thesis Assistance
If you would like Paul Mihas to provide feedback regarding a master’s thesis or dissertation proposal or draft of a chapter, please feel free to contact him at [email protected] .
Qualitative Data Analysis Software
The Odum Institute provides specialized computer programs that provide tools for mixed methods analyses; these include QSR NVivo, ATLAS.ti, MAXQDA, and a web-based program, Dedoose .
Odum offers short courses on these programs as well as consultations regarding their use. Please see the current Institute short course schedule or contact Paul Mihas to arrange a customized presentation for graduate or undergraduate classes or other special audiences.
QRS NVivo is a software program for coding and analyzing textual and multimedia data . It also allows researchers to construct diagrams (“mind maps” and “concept maps”) of codes and transcripts and automatically generates comparison diagrams to assess differences between codes or transcripts.
Its analytical strengths include:
- Cluster analysis of transcripts and multidimensional matrix analysis of codes
- Quantitative variables for “mixing” quantitative and qualitative data.
ATLAS.ti , a program for analyzing textual and multimedia data , allows users to analyze data based on codes and analytical memos . The software also allows users to create diagrams of transcripts, quotations, memos, and codes and to create links between these “objects” in diagrams.
The query tool lets users ask complex questions of their data, including Boolean searches or queries based on demographics. A co-occurrence table allows researchers to review conceptual intersections of codes. A joint-display matrix allows users to combine qualitative codes and quantitative variables.
MAXQDA is a qualitative analysis software package that helps researchers code textual, audio, or video data and analyze coded segments .
The software also allows users to merge qualitative and quantitative analysis by exporting and importing variables to and from SPSS and Excel. The software includes a mixed methods set of tools for generating tables that “mix” the qualitative codes and quantitative variables. A memo-writing feature allows users to add reflective writing to their analytic process.
A content analysis feature allows researchers to create a special dictionary of keywords. Intercoder reliability features are also available.
Dedoose is a web-based application for analyzing qualitative and mixed methods research with text, images, audio, videos, and spreadsheet data . The program provides numerous user-friendly charts for making sense of mixed methods studies.
Learning Opportunities
Qualitative research summer intensive:.
The Odum Institute has joined ResearchTalk, Inc. , in presenting the Qualitative Research Summer Intensive , a five-day qualitative research professional development course series, offered annually in July. The intensive includes courses on qualitative traditions, research design, data collection, analysis, and innovative strategies in the field.
Examples & Resources
Consultants at the Odum Institute have authored several online articles regarding specific qualitative methods. For more information, please visit the Sage website regarding learning to use:
Grounded Theory jQuery(document).ready(function(){ jQuery('.osc_tooltip').tooltip({ template:' ' }).on('shown.bs.tooltip', function(){ jQuery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'false'); }).on('hidden.bs.tooltip', function(){ jQuery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'true'); }); });
Phenomenological analysis jquery(document).ready(function(){ jquery('.osc_tooltip').tooltip({ template:'' }).on('shown.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'false'); }).on('hidden.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'true'); }); });, analyze written text jquery(document).ready(function(){ jquery('.osc_tooltip').tooltip({ template:'' }).on('shown.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'false'); }).on('hidden.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'true'); }); });, narrative analysis jquery(document).ready(function(){ jquery('.osc_tooltip').tooltip({ template:'' }).on('shown.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'false'); }).on('hidden.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'true'); }); });, build a codebook jquery(document).ready(function(){ jquery('.osc_tooltip').tooltip({ template:'' }).on('shown.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'false'); }).on('hidden.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'true'); }); });, charmazian grounded theory jquery(document).ready(function(){ jquery('.osc_tooltip').tooltip({ template:'' }).on('shown.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'false'); }).on('hidden.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'true'); }); });, visual analysis jquery(document).ready(function(){ jquery('.osc_tooltip').tooltip({ template:'' }).on('shown.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'false'); }).on('hidden.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'true'); }); });, analyze oral discourse jquery(document).ready(function(){ jquery('.osc_tooltip').tooltip({ template:'' }).on('shown.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'false'); }).on('hidden.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'true'); }); });, instrument development jquery(document).ready(function(){ jquery('.osc_tooltip').tooltip({ template:'' }).on('shown.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'false'); }).on('hidden.bs.tooltip', function(){ jquery( '.tooltip.oscitas-bootstrap-container' ).attr( 'aria-hidden', 'true'); }); });.
The Qualitative Research Resources Page from the UNC Health Sciences Library is also an excellent resource for information on qualitative research methods.
Qualitative Research Certificate
Graduate Certificate
The Qualitative Research Certificate consists of four three-credit hour courses (12 credit hours) developed to prepare students and professionals to understand a broad and in-depth knowledge of qualitative research approaches and to conduct qualitative research studies.
Over recent years, qualitative research has been increasingly conducted and influential in educational research across disciplines.
The Qualitative Research Certificate within the College of Education at Purdue University requires students to obtain a minimum grade of B for each course while also maintaining an overall GPA of 3.0/4.0. This certificate program accepts applications from Purdue University graduate students from any Purdue West Lafayette graduate programs.
This residential program has rolling admission. Applications must be fully complete and submitted (including all required materials) and all application fees paid prior to the deadline in order for applications to be considered and reviewed. For a list of all required materials for this program application, please see the “Admissions” tab below.
July 1 is the deadline for Fall applications.
November 15 is the deadline for Spring applications.
March 15 is the deadline for Summer applications.
This program does not lead to licensure in the state of Indiana or elsewhere. Contact the College of Education Office of Teacher Education and Licensure (OTEL) at [email protected] before continuing with program application if you have questions regarding licensure or contact your state Department of Education about how this program may translate to licensure in your state of residence.
Application Instructions for the Qualitative Research Certificate from the Office of Graduate Studies :
In addition to a submitted application (and any applicable application fees paid), the following materials are required for admission consideration, and all completed materials must be submitted by the application deadline in order for an application to be considered complete and forwarded on to faculty and the Purdue Graduate School for review.
Here are the materials required for this application:
- Official, current Purdue transcripts
- Graduate School Form 18 for Dual Enrolled students. Please upload this form with your application with your signature and information only. Our office will obtain the necessary faculty signatures.
- Academic Statement of Purpose
- Personal History Statement
We encourage prospective students submit an application early, even if not all required materials are uploaded. Applications are not forwarded on for faculty review until all required materials are uploaded.
When submitting your application for this program, please select the following options:
- Select a Campus: Purdue West Lafayette (PWL)
- Select your proposed graduate major: Curriculum and Instruction
- Please select an Area of Interest: Curriculum Studies
- Please select a Degree Objective: Qualitative Research Graduate Certificate
- Primary Course Delivery: Residential
Program Requirements
Required courses.
- EDCI 61500: Qualitative Research Methods in Education (3 cr.) A course providing an introduction to qualitative research methods in education.
- EDCI 61600: Qualitative Data Collection and Analysis in Educational Research (3 cr.) A course focused on collection and analysis of qualitative data
- Elective #1: with focus on qualitative methods (3 cr.)
- Elective #2: with focus on qualitative methods (3 cr.)
- CAND 99100: Candidate (Must be registered as a candidate for graduation to receive the Certificate) Candidate registration should be completed through the Office of Graduate Studies when registering for the final course. Student must contact the office directly at [email protected] . Failure to register properly will result in a delay of being awarded the certificate
- EDCI 567: Action Research in Science Education
- EDCI 59100: Research in International Contexts
- EDCI 591: Technology for Qualitative Research
- EDCI 612: Literacy Research Methodologies
- ANTH 605: Seminar in Ethnographic Analysis
- COM 584: Historical/Critical Research in Communication
- HDFS 679: Qualitative Research on Families
- TECH 697: Qualitative Research Methods in Technology Studies
- WGSS 680: Feminist Theory
- WGSS 682: Issues in Feminist Research and Methodology
- Other elective courses may be approved (before completing) by the faculty advisor in the home department in conjunction with the Qualitative Research Certificate coordinator in the Dept. of Curriculum and Instruction
APPLICATION PROCEDURE
Course Content Information or Blackboard: Contact Dr. Stephanie Zywicki Course Registration, payment, drops/withdraws, and removing holds: [email protected] Career accounts: ITaP (765) 494-4000
- Student Login
- Instructor Login
- Areas of Study
- Art and Design
- Behavioral Health Sciences
- Business Administration
- Leadership and Management
- Project Management
- See the full list
- Construction and Sustainability
- Humanities and Languages
- Mathematics and Statistics
- Sciences and Biotechnology
- Chemistry and Physics
- Clinical Laboratory Science
- Health Advising
- Life Science Business and Biotechnology
- Online Sciences Courses
- Technology and Information Management
- Writing, Editing and Technical Communication
- Transfer Credit
- Transfer Credit Courses
- Online Learning
- Online Courses and Certificates
- Information Sessions
- Career Services
- Career-Development Courses
- Professional Internship Program
- Custom Programs
- For Universities and Organizations
- Academic Services
- Transcripts
- General Information
- Community Guidelines
- Course and Program Information
- Latest COVID-19 Information
- Online Course Policies
- Certificates, Programs and CEUs
- Concurrent Enrollment
- International Student Services
- Student Aid
- Disability Support Services
- Financial Assistance
- Voices Home
- Educator Insights
- Student Stories
- Professional Pathways
- Industry Trends
- Free and Low Cost Events
- Berkeley Global
Qualitative Research: Design, Implementation and Methods
DESIGN X440.2
Get an introduction to what qualitative research is, the types of qualitative research methods, the appropriate situations to apply qualitative methods, and how to conduct your own qualitative research. You learn to build a research protocol and use various techniques to design, conduct, analyze and present an informative research study.
At the end of the course, you are expected to conduct your own qualitative research study . To that end, you develop a research plan based on the given situation, collect data using qualitative methodologies , engage with various techniques for coding and analyzing qualitative data effectively, and present the data and insights in a manner that is best aligned with the goals of the research.
Prerequisites: None.
Course Outline
Course Objectives
- Understand what constitutes qualitative research, how it differs from quantitative research and when to apply qualitative research methods
- Identify and formulate appropriate qualitative research plans
- Apply qualitative research data collection techniques
- Develop coding schemes for analysis of qualitative data
- Present qualitative data to inform and influence
What You Learn
- Developing qualitative research questions
- Building a research protocol
- Observing, listening and probing: the core skills of a qualitative researcher
- Qualitative sampling and participant recruitment
- Understanding an overview of the qualitative data analysis process
- Communicating your findings, from summary to interpretation
- Presenting qualitative results
How You Learn
We are online! All of the design classes are conducted online and include video classes, mentor-led learning and peer-to-peer support through our student online platform, Canvas.
- Reading assignments
- Quizzes at instructor’s discretion
- Small-group activities
- Homework assignments
- Capstone project
Is This Course Right for You?
This course is intended for students in the Professional Program in User Experience (UX) Design , or anybody interested in obtaining skills in qualitative research. You do not need preexisting research experience for this course. Our experienced instructors provide practical information, leverage their qualitative research skills and monitor your development along with peer-to-peer support on our student online platform.
Summer 2024 enrollment opens on March 18!
Thank you for your interest in this course!
The course you have selected is currently not open for enrollment.
Enter your email below to be notified when it becomes available.
Required Field
Get Notified
We're excited that you have chosen us as your education provider.
Once a section for this class is available, we will email you with enrollment information.
Your privacy is important to us .
Email Privacy Policy
Your privacy is important to us!
We do not share your information with other organizations for commercial purposes.
We only collect your information if you have subscribed online to receive emails from us.
We do not partner with or have special relationships with any ad server companies.
If you want to unsubscribe, there is a link to do so at the bottom of every email.
Read the full Privacy Policy
← Back to your information .
Session Time-Out
Privacy policy, cookie policy.
This statement explains how we use cookies on our website. For information about what types of personal information will be gathered when you visit the website, and how this information will be used, please see our Privacy Policy .
How we use cookies
All of our web pages use "cookies". A cookie is a small file of letters and numbers that we place on your computer or mobile device if you agree. These cookies allow us to distinguish you from other users of our website, which helps us to provide you with a good experience when you browse our website and enables us to improve our website.
We use cookies and other technologies to optimize your website experience and to deliver communications and marketing activities that are targeted to your specific needs. Some information we collect may be shared with selected partners such as Google, Meta/Facebook or others. By browsing this site you are agreeing to our Privacy Policy . You can revoke your voluntary consent to participate in monitored browsing and targeted marketing by selecting “Disable All Cookies” below.
Types of cookies we use
We use the following types of cookies:
- Strictly necessary cookies - these are essential in to enable you to move around the websites and use their features. Without these cookies the services you have asked for, such as signing in to your account, cannot be provided.
- Performance cookies - these cookies collect information about how visitors use a website, for instance which pages visitors go to most often. We use this information to improve our websites and to aid us in investigating problems raised by visitors. These cookies do not collect information that identifies a visitor.
- Functionality cookies - these cookies allow the website to remember choices you make and provide more personal features. For instance, a functional cookie can be used to remember the items that you have placed in your shopping cart. The information these cookies collect may be anonymized and they cannot track your browsing activity on other websites.
Most web browsers allow some control of most cookies through the browser settings. To find out more about cookies, including how to see what cookies have been set and how to manage and delete them please visit https://www.allaboutcookies.org/.
Specific cookies we use
The list below identify the cookies we use and explain the purposes for which they are used. We may update the information contained in this section from time to time.
- JSESSIONID: This cookie is used by the application server to identify a unique user's session.
- registrarToken: This cookie is used to remember items that you have added to your shopping cart
- locale: This cookie is used to remember your locale and language settings.
- cookieconsent_status: This cookie is used to remember if you've already dismissed the cookie consent notice.
- _ga_UA-########: These cookies are used to collect information about how visitors use our site. We use the information to compile reports and to help us improve the website. The cookies collect information in an anonymous form, including the number of visitors to the website, where visitors have come to the site from and the pages they visited. This anonymized visitor and browsing information is stored in Google Analytics.
Changes to our Cookie Statement
Any changes we may make to our Cookie Policy in the future will be posted on this page.

Short courses

Qualitative Research Methods in Health
- 10am - 1pm each day
Cost: £1,500
Book a place.
Please email [email protected] if you wish to apply for this course. The next course will start on 3 October 2024
This course aims to equip you with the knowledge and skills to understand, design and conduct high quality qualitative research.
The course will help you:
- gain a clear understanding of the principles of qualitative research
- practise skills including interviewing, running a focus group, data analysis, and developing and presenting a research protocol
This course will be delivered online over 10 Thursday mornings from 3 October to 12 December.
This course is run by researchers from the UCL Centre for Excellence in Qualitative Research, within the Research Department of Primary Care and Population Health (PCPH).
Who it's for
This course is for:
- Master's level students, PhD students and research staff who need to design and conduct a qualitative study
- those who wish to know how to assess the quality of qualitative research (e.g. funders, journal editors, ethical committee members etc.)
You don't need to have any previous experience of qualitative research, but you will need to do some preparation before each session.
Course content
Lead: Julia Bailey and Tom Witney
This workshop will help you understand the basis on which qualitative methodology is selected as a research approach.
- learn about the philosophical debates around qualitative research
- contrast qualitative and quantitative approaches
- discuss the place of qualitative research in health and medicine
You'll also critique a published paper of a qualitative study. This will help you reflect on a completed study and consider not only the methodological approach and selection of methods, but also practical aspects such as sampling, what counts as data, the position of the researcher, data analysis, and application of findings.
Learning objectives
By the end of this workshop you'll be able to:
- describe key features of qualitative research
- explain the rationale for key features of qualitative research design
- know when qualitative or quantitative study designs are appropriate
- understand how ‘theory’ is relevant for qualitative research
Leads: Harpreet Sihre and Silvie Cooper
On this workshop you'll learn about qualitative research interviewing techniques and developing topic guides.
You'll explore structured, semi-structured and in-depth interview methods and their application, using real world examples. However, the emphasis will be on semi-structured interview techniques.
You'll also learn about and discuss:
- the importance of different communication styles and researcher reflexivity
- practical issues such as structuring questions, building rapport and dealing with challenging interviews
You'll be encouraged to think of an area of research around which you'll structure and produce a topic guide for use in a practical session. You'll also get the opportunity to practice your newly developed interviewing skills.
As far as possible, the workshop is tailored towards research that those attending are planning/doing.
By the end of this workshop you'll be able to:
- describe and distinguish between structured, semi-structured and 'in-depth' interviewing
- formulate and construct a topic guide
- apply and evaluate some key interviewing skills
Lead: Tom Witney and Fiona Aspinal
This workshop will introduce you to focus groups - a key qualitative research method.
You'll learn about the:
- different stages of the research process where focus groups can be used
- types of research questions that lend themselves to this approach
- practicalities of sampling, convening and conducting focus groups, including issues to consider when researching sensitive topics
You'll also practise your communication and group facilitation skills.
You'll be encouraged to think of an area of research around which you'll structure and produce a topic guide for use in a practical session.
- explain when and how to use focus groups
- design a topic guide for a focus group study
- organise and facilitate a focus group
Leads: Nathan Davies and Fiona Stevenson
On this workshop you'll discuss a range of ways of conducting qualitative data analysis and the rationales for different approaches.
You'll be encouraged to critically reflect on how decisions made throughout research affect the type and extent of analysis possible. The importance of decisions about transcription are also stressed.
You'll consider the place of data management software in qualitative analysis. You won't be taught how to use particular software packages, but you'll discuss the advantages and disadvantages of using these.
You'll conduct a thematic analysis on a piece of data, and reflect on and consider the best approach for your own work.
Please note: this workshop does not provide training in the use of Computer Assisted Qualitative Data Analysis packages
- distinguish between different types of qualitative data analysis
- recognise the importance of decisions relating to transcribing, reflexivity, field notes, double coding and data management
- consider various approaches to analysis
- understand the principles and practicalities of conducting a basic thematic analysis
- evaluate the benefits of Computer Assisted Qualitative Data Analysis for your projects
Leads: Jane Wilcock and Stephanie Kumpunen
In this interactive workshop you'll plan your own qualitative study design.
You'll work on your own and in small and large groups, with an experienced tutor. You'll also have the opportunity for one-to-one and small group discussions and advice on qualitative study design.
The first day is spent planning your study in a structured way. On the second day you'll present your study design proposal to tutors and other students in small groups, and discuss research issues arising from the proposed studies.
- write clear research questions
- understand the principles of (and debates about) quality in qualitative research
- plan a qualitative research study, specifying the details of how a study will be carried out
- present a four-slide summary of your study design
- discuss the rationale for chosen study designs
Teaching and assessment
The course is highly interactive, involving a range of teaching techniques including group work, practical tasks and discussion.
It will be run with a mixture of synchronous, online learning (e.g. presentations, small group discussions) and asynchronous learning (pre-recorded videos, readings, preparatory writing/planning).
You'll receive help designing and planning your own qualitative research project. You'll then present your design proposals and receive feedback from course tutors and peers at the end of the course.
You'll be required to do some preparation before each session (reading and/or watching videos).
How to apply
To apply for this course you’ll need to complete a short application form.
Your application will be judged on your suitability for the course and how much you're likely to benefit. Priority will be given to people who are actively planning or conducting qualitative research.
Please email [email protected] if you’d like to be added to the waiting list. When booking opens and there are spaces available for the course, you'll be emailed the application form.
Cancellation policy
Cancellations must be received in writing at least two weeks before the start of the event and will be subject to an administration charge of 20% of the course fee. Unfortunately, no refunds will be made within two weeks of the course date. Any refund will be made by UCL to you within 30 days of your cancellation and be paid to you in the same way as you paid for your order.
We reserve the right to cancel teaching if necessary and will, in such event, make a full refund of the registration fee. PCPH Events will not be liable for any additional incurred costs.
Further information
If you have any questions about the course content, please email Fiona Stevenson ( [email protected] ) or Julia Bailey ( [email protected] ).
For administrative queries, please contact Lynda Russell-Whitaker ( [email protected] ).
Course team

Julia Bailey - joint Course Director
Julia is an Associate Professor at the e-Health Unit at UCL and a sexual health speciality doctor in South East London. Her research interests include sexual health, e-Health, doctor-patient interaction, science communication and social science in medicine (qualitative methodologies). View Julia’s IRIS profile for more information about her work and publications.

Fiona Stevenson - joint Course Director
Fiona is a Professor of Medical Sociology and Co-Director of e-Health Unit at UCL. She’s currently Head of the Department of Primary Care and Population Health at UCL. Her research is broadly encompassed by the overarching theme of perceptions, communication and interactions about treatment. Her methodological expertise lies in qualitative methods, both in relation to thematic analysis of interviews and focus groups and conversation analysis of interactional data. She has expertise in conducting original research as well as implementing research findings into practice. View Fiona’s IRIS profile for more information about her work and publications.

Nathan Davies
Nathan is an Associate Professor and Alzheimer’s Society Fellow based in the Centre for Ageing Population Studies at UCL. His main research interests are in older adults, dementia, and supporting family carers. He's a qualitative researcher leading on several qualitative studies, which explore sensitive topics, including end of life care. In addition to experience of interviews, focus groups and various types of qualitative analysis, he has extensive experience of co-design, co-production and consensus-based methods. View Nathan’s IRIS profile for more information about his work and publications.

Jane Wilcock
Jane is a Senior Research Associate in the Centre for Ageing & Population Studies, UCL. Her main research interests are in dementia, ageing, emergent technologies and trials of complex interventions in primary care and community settings. A mixed-methods researcher, Jane has experience of a variety of study designs such as RCTs, interview and focus group studies, nominal group techniques and co-design of interventions. In addition, she is a methodology expert for the NIHR Research Design Service London. View Jane’s IRIS profile for more information about her work and publications.

Silvie Cooper
Silvie is a Lecturer (Teaching) in the Department of Applied Health Research at UCL. Her research interests include capacity building for health research, management of chronic pain, digital health, and patient education, using qualitative, mixed methods, and translational research approaches. Alongside her research, she designs and teaches on a variety of health and social science courses for undergraduates, postgraduates and professionals. Topics include research and evaluation methods, the social aspects of health and illness, and the impact of context, practice and policy on healthcare experiences. View Silvie’s IRIS profile for more information about her works and publications.

Harpreet Sihre
Harpreet formerly completed her PhD at the Institute of Applied Health Research, University of Birmingham, where she researched the lived experiences of South Asian women with severe postnatal psychiatric illnesses using Interpretative Phenomenological Analysis. She then worked at the Unit of Social and Community Psychiatry on an NIHR-funded study researching accessibility and acceptability of Perinatal Mental Health Services.
Harpreet’s research interests encompass mental health, perinatal mental health, access to services and equality, diversity and inclusion, using qualitative research methods. Harpreet has taught on both undergraduate and postgraduate courses, including small group teaching and lecturing at the University of Birmingham and Queen Mary University. View Harpreet’s IRIS profile for more information about her work and publications.

Tom is a Research Fellow at the department of Primary Care and Population Health . He is a qualitative health researcher, with a particular interest in sexual health and relationship intimacy. His current work focuses on improving access to sexual health for trans and gender diverse people and supporting uptake of chlamydia retesting following a diagnosis. View Tom’s Iris profile for more information about his work and publications.

Fiona Aspinal
Fiona is based in the Department of Applied Health Research for the NIHR ARC North Thames as 'Senior Research Associate in Qualitative Methods Applied to Organisational Research in Health' where, as part of the ARC North Thames' Research Partnership Team, she helps to facilitate and support health and social care research with local, regional and national relevance. She is also the social care research lead for NIHR CRN North Thames.
Her areas of research interest are: Qualitative research and evaluation of complex health and social care interventions and organisations; The experience and outcomes of integrated care policy and practice for staff, service users and informal carers; Social and community health care for adults, including people with dementia; Social care research infrastructure/skills.
At UCL, in addition to the Qualitative Research Methods in Health short course, Fiona teaches on research methods and social science courses and modules, such as the BSc Population Health Sciences, the Medicine MBBS BSc and the Population Health MSc. She also supervises undergraduate and postgraduate students. View Fiona’s Iris profile for more information about her work and publications.

Stephanie Kumpunen
Stephanie is a THIS Institute Doctoral Fellow at UCL and a Senior Fellow in Health Policy at Nuffield Trust (a London-based health and care think tank). Her research focuses on the organisation of Primary Care and community-based health and care services.
Stephanie has led on a number of qualitative studies and mixed-methods evaluations. She has a particular interest in rapid qualitative approaches; namely rapid ethnographies that inform health and care service improvement. View Stephanie’s UCL profile for more information about her work and publications.
“The course is a really a great opportunity to read, reflect, discuss and share research, which is helpful for personal and professional development.” [Academic Clinical Fellow, Spring 2022]
“This session really helped me to organise my thoughts and put together a coherent plan for future research. It will make writing my protocol very easy!” [PhD Student, Spring 2022]
“It was such an excellent course. The information and materials provided were straight to the point and helpful, the working atmosphere was inspiring and constructive, and the tasks were interesting and activating. Thank you to all tutors!” [Clinical Research Programme Coordinator, Spring 2022]
“Great tutors, great reading material. It was very interesting to hear other peoples' experiences. Although this course was virtual, there were plenty of opportunities for interaction. I now have a better understanding and I am confident to run my study. I would recommend this course to anyone who wants an intro in qual research.” [Pre-Doctoral Research Fellow, 2021]
"I have a more clear understanding of the basics of qual methods, terminology and ways it may fit into my own research." [Researcher, 2019]
Course information last modified: 22 Apr 2024, 13:33
Length and time commitment
- Time commitment: 10am - 1pm each day
- Course length: 10 weeks
Contact information
- Lynda Russell-Whitaker
- [email protected]
Related Short Courses

NCRM delivers training and resources at core and advanced levels, covering quantitative, qualitative, digital, creative, visual, mixed and multimodal methods
20th Anniversary Impact Prize
Tell us how NCRM has helped you to make an impact

Short courses
Browse our calendar of training courses and events

Featured training course

Our resources
NCRM hosts a huge range of online resources, including video tutorials and podcasts, plus an extensive publications catalogue.

Online tutorials
Access more than 80 free research methods tutorials

Resources for trainers
Browse our materials for teachers of research methods
Methods News

NCRM annual lecture to explore AI in social research

Contribute to MethodsCon: Futures

Applications open for NCRM 20th Anniversary Impact Prize
10 free data analytics courses you can take online

Data analytics is the science of taking raw data, cleaning it, and analyzing it to inform conclusions and support decision making. From business to health care to social media, data analytics is changing the way organizations operate.
“It’s not hyperbole to say that data analytics has really taken over the world,” says Brian Caffo, professor of biostatistics at Johns Hopkins University’s Bloomberg School of Public Health and director of academic programs for the university’s Data Science and AI Institute. “Every domain has become increasingly quantitative to inform decision making.”
Berkeley's Data Science Master's
And this space isn’t slowing down anytime soon: The U.S. Bureau of Labor Statistics projects that employment for data scientists will grow 35% from 2022 to 2032, with 17,700 new job openings projected each year on average during that decade.
Interested in becoming a data analyst? Below, we’ve compiled ten free data analytics courses to help give you a firmer grasp of this rapidly growing field.
A/B Testing
About: This course covers the design and analysis of A/B tests, which are online experiments that compare two versions of content to see which one appeals to viewers more. A/B tests are used throughout the tech industry by companies like Amazon and Google. This course is offered through Udacity.
Course length: Six self-paced modules
Who this course is for: Beginners
What you’ll learn: In this course you’ll learn about A/B testing, experiment ethics, how to choose metrics, design an experiment, and analyze results.
Prerequisites: None
Data Analytics Short Course
About: In this quick, five-tutorial course you’ll get a broad overview of data analytics. You’ll learn about the different types of roles in data analytics, a summary of the tools and skills you’ll need to develop, and a hands-on introduction to the field. This course is offered by CareerFoundry.
Course length: 75 minutes, divided into five 15-minute lessons
What you’ll learn: In this course you’ll get an introduction to data analytics. You’ll also analyze a real dataset to solve a business problem through data cleaning, visualizations, and garnering final insights.
Prerequisites: None
Data Science: R Basics
About: This program gives you a foundational knowledge of programming language R. Offered by HarvardX through the EdX platform, this course is offered for free; the paid version includes a credential. It’s the first of ten courses HarvardX offers as part of its Professional Certificate in Data Science.
Course length: Eight weeks, 1–2 hours per week
What you’ll learn: In this course you’ll learn basic R syntax and foundational R programming concepts, including data types, vectors arithmetic, and indexing. You’ll also perform operations that include sorting, data wrangling using dplyr, and making plots.
“It’s the basics of how to wrangle, analyze, and visualize data in R,” says Dustin Tingley, Harvard University’s deputy vice provost for advances in learning and a professor of government in the school’s government department. “That gets you writing a little bit of code, but you’re not doing anything that heavy.”
Prerequisites: HarvardX recommends having an up-to-date browser to enable programming directly in a browser-based interface
Fundamentals of Qualitative Research Methods
About: This course will teach you the fundamentals of qualitative research methods. Qualitative research provides deeper insights into real-world problems that might not always be immediately evident. This course is offered through Yale University on YouTube.
Course length: 90 minutes spread out over six modules
What you’ll learn: In this course you’ll learn how qualitative research is a way to systematically collect, organize, and interpret information that is difficult to measure quantitatively. This includes developing qualitative research questions, gathering data through interviews and focus groups, and analyzing this data.
“Qualitative research is the systematic, rigorous application of narratives and tools to better understand a complex phenomenon,” says Leslie Curry, a professor of public health and management at the Yale School of Public Health and a professor of management at the Yale School of Management. She adds that this approach can help understand flaws in large data sets. “It can be used as an adjunct to a lot of the really important work that’s happening in large data analysis.”
Getting and Cleaning Data
About: This course covers the basic ways that data can be obtained and how that data can be cleaned to make it “tidy.” It will also teach you the components of a complete data set, such as raw data, codebooks, processing instructions, and processed data. This course is offered by Johns Hopkins University through Coursera, and is part of a 10-course Data Science Specialization series.
Course length: Four weeks, totaling approximately 19 hours
What you’ll learn: Through this course you’ll learn about common data storage systems, how to use R for text and date manipulation, how to use data cleaning basics to make data “tidy,” and how to obtain useable data from the web, application programming interfaces (APIs), and databases.
“It’s the starting point” when it comes to data analysis, Caffo says. “Without a good data set that is cleaned and appropriate for use, you have nothing. You can talk all you want about doing models or whatnot—underlying that has to be the data to support it.”
Prerequisites: None
Introduction to Data Science with Python
About: This course teaches you concepts and techniques to give you a foundational understanding of data science and machine learning. Offered by HarvardX through the EdX platform, this course can be taken for free. The paid version offers a credential.
Course length: Eight weeks, 3–4 hours a week
Who this course is for: Intermediate
What you’ll learn: This course will give you hands-on experience using Python to solve real data science challenges. You’ll use Python programming and coding for modeling, statistics, and storytelling.
“It gets you up and running with the main workhorse tools of data analytics,” says Tingley. “It helps to set people up to take more advanced courses in things like machine learning and artificial intelligence.”
Prerequisites: None, but Tingley says having a basic background in high school-level algebra and basic probability is helpful. Some programming experience—particularly in Python—is recommended
Introduction to Databases and SQL Querying
About: In this course you’ll learn how to query a database, create tables and databases, and be proficient in basic SQL querying. This free course is offered through Udemy.
Course length: Two hours and 17 minutes
What you’ll learn: This course will acquaint you with the basic concepts of databases and queries. This course will walk you through setting up your environment, creating your first table, and writing your first query. By the course’s conclusion, you should be able to write simple queries related to dates, string manipulation, and aggregation.
Introduction to Data Analytics
About: This course offers an introduction to data analysis, the role of a data analyst, and the various tools used for data analytics. This course is offered by IBM through Coursera.
Course length: Five modules totaling roughly 10 hours
What you’ll learn: This course will teach you about data analytics and the different types of data structures, file formats, and sources of data. You’ll learn about the data analysis process, including collecting, wrangling, mining, and visualizing data. And you’ll learn about the different roles within the field of data analysis.
Learn to Code for Data Analysis
About: This course will teach you how to write your own computer programs, access open data, clean and analyze data, and produce visualizations. You’ll code in Python, write analyses and do coding exercises using the Jupyter Notebooks platform. This course is offered through the United Kingdom’s Open University on its OpenLearn platform.
Course length: Eight weeks, totaling 24 hours
What you’ll learn: In this course you’ll learn basic programming and data analysis concepts, recognize open data sources, use a programming environment to develop programs, and write simple programs to analyze large datasets and produce results.
Prerequisites: A background in coding—especially Python—is helpful
The Data Scientist’s Toolbox
About: This course will give you an introduction to the main tools and concepts of data science. You will learn the ideas behind turning data into actionable knowledge and get an introduction to tools like version control, markdown, git, GitHub, R, and RStudio. This course is offered by Johns Hopkins University through Coursera, and is part of a 10-course Data Science Specialization series.
Course length: 18 hours
What you’ll learn: This course will teach you how to set up R, RStudio, GitHub, and other tools. You will learn essential study design concepts, as well as how to understand the data, problems, and tools that data analysts use.
“That course is a very accessible introduction for anyone who wants to get started in this,” Caffo says. “It’s an overview that covers the full pipeline, from things like collecting and arranging data to asking good questions, all the way to creating a data deliverable.”
The takeaway
From businesses estimating demand for their products to political campaigns figuring out where they should run advertisements to health care professionals running clinical trials to judge a drug’s efficacy, data analytics has a wide variety of applications. Getting a better understanding of the field on your own time can be done easily and freely. And the field is only growing.
“Just about every field is having a revolution in data analytics,” Caffo says. “In fields like medicine that have always been data driven, it’s become more data-driven.”
Syracuse University MS in Applied Data Science Online
Mba rankings.
- Best Online MBA Programs for 2024
- Best Online Master’s in Accounting Programs for 2024
- Best MBA Programs for 2024
- Best Executive MBA Programs for 2024
- Best Part-Time MBA Programs for 2024
- 25 Most Affordable Online MBAs for 2024
- Best Online Master’s in Business Analytics Programs for 2024
Information technology & data rankings
- Best Online Master’s in Data Science Programs for 2024
- Most Affordable Master’s in Data Science for 2024
- Best Master’s in Cybersecurity Degrees for 2024
- Best Online Master’s in Cybersecurity Degrees for 2024
- Best Online Master’s in Computer Science Degrees for 2024
- Best Master’s in Data Science Programs for 2024
- Most Affordable Online Master’s in Data Science Programs for 2024
- Most Affordable Online Master’s in Cybersecurity Degrees for 2024
Health rankings
- Best Online MSN Nurse Practitioner Programs for 2024
- Accredited Online Master’s of Social Work (MSW) Programs for 2024
- Best Online Master’s in Nursing (MSN) Programs for 2024
- Best Online Master’s in Public Health (MPH) Programs for 2024
- Most Affordable Online MSN Nurse Practitioner Programs for 2024
- Best Online Master’s in Psychology Programs for 2024
Leadership rankings
- Best Online Doctorate in Education (EdD) Programs for 2024
- Most Affordable Online Doctorate in Education (EdD) Programs for 2024
- Coding Bootcamps in New York for 2024
- Best Data Science and Analytics Bootcamps for 2024
- Best Cybersecurity Bootcamps for 2024
- Best UX/UI bootcamps for 2024
Boarding schools
- World’s Leading Boarding Schools for 2024
- Top Boarding School Advisors for 2024
Earn Your Master’s in Data Science Online From SMU
Effectiveness of Psychosocial Skills Training and Community Mental Health Services: A Qualitative Research
- Original Paper
- Published: 22 April 2024
Cite this article

- Halil İbrahim Bilkay ORCID: orcid.org/0000-0002-8231-960X 1 ,
- Burak Şirin ORCID: orcid.org/0000-0002-8485-5756 2 &
- Nermin Gürhan ORCID: orcid.org/0000-0002-3472-7115 2
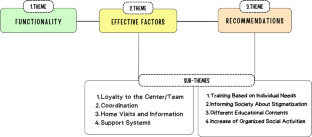
This study employs a phenomenological approach to investigate the experiences of individuals who access services at a community mental health center (CHMC) in Türkiye The aim of this study is to comprehend the experiences of individuals who participate in psychosocial skills training at the CHMC. Thematic analysis of data from sixteen in-depth interviews revealed three main themes and eight sub-themes. Functionality theme emphasizes the positive impact of CHMC services and training on daily life and social functioning. Effective Factors theme encompasses the elements that improve the effectiveness of CHMC services. Participants have provided suggestions for the content of the training under the theme of Recommendations. Study results show that CHMC services and psychosocial skills training benefit individuals' daily lives and functioning, but that opportunities for improvement exist. It is crucial to incorporate participant feedback, and further research should be conducted to investigate the effectiveness of these services in this area.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
Similar content being viewed by others

Piloting a mental health training programme for community health workers in South Africa: an exploration of changes in knowledge, confidence and attitudes
Goodman Sibeko, Peter D. Milligan, … Dan J. Stein

The experiences of lay health workers trained in task-shifting psychological interventions: a qualitative systematic review
Ujala Shahmalak, Amy Blakemore, … Waquas Waheed
“These are people just like us who can work”: Overcoming clinical resistance and shifting views in the implementation of Individual Placement and Support (IPS)
Danika Sharek, Niamh Lally, … Agnes Higgins
Abaoglu, H., Mutlu, E., Ak, S., Akı, E., & Anıl Yagcıoglu, E. (2020). The effect of life skills training on functioning in schizophrenia: A randomized controlled trial. Schizophrenia Bulletin, 46 (Suppl 1), S220. https://doi.org/10.1093/schbul/sbaa030.533
Article PubMed Central Google Scholar
Alatas, G., Karaoglan, A., Arslan, M. ve Yanik, M. (2009). Toplum temelli ruh sağlığı modeli ve Türkiye’de toplum ruh sağlığı merkezleri projesi. Nöropsikiyatri Arşivi, 46 (Özel Sayı), 25–29.
Aruldass, P., Sekar, T. S., Saravanan, S., Samuel, R., & Jacob, K. S. (2022). Effectiveness of social skills training groups in persons with severe mental illness: A pre–post intervention study. Indian Journal of Psychological Medicine, 44 (2), 114–119. https://doi.org/10.1177/02537176211024146
Article PubMed Google Scholar
Attepe Ozden, S., Tekindal, M., Gedik, T. E., Ege, A., Erim, F. & Tekindal, M. A. (2022). Reporting qualitative research: Turkish adaptation of COREQ checklist. European Journal Of Science And Technology, (35), 522–529. https://doi.org/10.31590/ejosat.976957
Aydin, M., Altınbaş, K., Nal, Ş, Ercan, S., Ayhan, M., Usta, A., & Özbek, S. (2019). The comparison of patients with schizophrenia in community mental health centers according to living conditions in nursing home or home. Anatolian Journal of Psychiatry., 21 (1), 14–23. https://doi.org/10.5455/apd.42123
Article Google Scholar
Bag, B. (2018). An example of a model for practicing community mental health nursing: recovery. Current Approaches in Psychiatry , 10 (4), 481–493. https://doi.org/10.18863/pgy.375814
Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health, 11 (4), 589–597. https://doi.org/10.1080/2159676X.2019.1628806
Bekiroglu, S., & Ozden, S. A. (2021). Psychosocial interventions for individuals with severe mental illness and their families in Turkey: A systematic review. Current Approaches in Psychiatry , 13(1), 52–76. https://doi.org/10.18863/pgy.721987
Chan, A., Wong, S., & Chien, W. (2018). A prospective cohort study of community functioning among psychiatric outpatients. Psychiatry Research, 259 , 125–134. https://doi.org/10.1016/j.psychres.2017.10.019
Creswell, J. W., & Creswell, J. D. (2017). Research design: Qualitative, quantitative, and mixed methods approaches (4th ed.). Sage.
Google Scholar
Creswell, J. W. (2013). Qualitative inquiry & research design: Choosing among five approaches . Sage.
Chronister, J., Fitzgerald, S., & Chou, C.-C. (2021). The meaning of social support for persons with serious mental illness: A family member perspective. Rehabilitation Psychology, 66 (1), 87–101. https://doi.org/10.1037/rep0000369
Corrigan, P. W., Morris, S. B., Michaels, P. J., Rafacz, J. D., & Rusch, N. (2012). Challenging the public stigma of mental illness: A meta-analysis of outcome studies. Psychiatric Services (Washington, D.C.), 63 (10), 963–973. https://doi.org/10.1176/appi.ps.201100529
Coker, F., Yalcınkaya, A., Celik, M., & Uzun, A. (2021). The effect of community mental health center services on the frequency of hospital admission, severity of disease symptoms, functional recovery, and insight in patients with schizophrenia. Journal of Psychıatrıc Nursıng , 12 (3):181–187 https://doi.org/10.14744/phd.2021.18199
De Mamani, A. W., Altamirano, O., McLaughlin, M., & Lopez, D. (2020). Culture and family-based intervention for schizophrenia, bipolar, and other psychotic-related spectrum disorders. Cross-Cultural Family Research and Practice , 645–674. https://doi.org/10.1016/b978-0-12-815493-9.00020-x
Ensari, H., Gultekin, B. K., Karaman, D., Koc, A., & Beskardes, A. F. (2013). The effects of the service of community mental health center on the patients with schizophrenia - evaluation of quality of life, disabilities, general and social functioning-a summary of one year follow-up. Anatolian Journal Psychiatry, 14 (82), 108-114. https://doi.org/10.5455/apd.36380
Fan, Y., Ma, N., Ouyang, A., Zhang, W., He, M., Chen, Y., Liu, J., Li, Z., Yang, J., Ma, L., & Caine, E. D. (2022). Effectiveness of a community-based peer support service among persons suffering severe mental illness in China. PeerJ, 10 , e14091. https://doi.org/10.7717/peerj.14091
Article PubMed PubMed Central Google Scholar
Guvenc, N. C., & Oner, H. (2020). Views of patient relatives and health professionals about the reasons of the patients enrolled in the community mental health center to discontinue or irregularly continue the center. The International Journal of Social Psychiatry, 66 (7), 707–723. https://doi.org/10.1177/0020764020931875
Houser, J. (2015). Nursing research: Reading, using, and creating evidence (3rd ed.). Jones and Bartlett Learning.
Lee, H. J., Ju, Y. J., & Park, E. C. (2017). Utilization of professional mental health services according to recognition rate of mental health centers. Psychiatry Research, 250 , 204–209. https://doi.org/10.1016/j.psychres.2017.01.051
Liberman, R. P., Wallace, C. J., Blackwell, G., Eckman, T. A., Vaccaro, J. V., & Kuehnel, T. G. (1993). Innovations in skills training for the seriously mentally ill: The UCLA social and independent living skills modules. Innovations and Research, 2 (2), 43–59.
Merriam, S. B. (2009). Qualitative research: A guide to design and implementation: Revised and expanded from qualitative research and case study applications in education . Jossey-Bass.
Picton, C. J., Moxham, L., & Patterson, C. (2017). The use of phenomenology in mental health nursing research. Nurse Researcher, 25 (3), 14–18. https://doi.org/10.7748/nr.2017.e1513
Polit, D. F., Beck, C. T. (2004). Nursing research principles & methods , 7th Edition. Williams & Wilkins, Chapter 13: 289–314.
Potash, J. (2019). Continuous acts of creativity: Art therapy principles of therapeutic change. Art Therapy, 36 , 173–174. https://doi.org/10.1080/07421656.2019.1684159
Rodriguez, A., & Smith, J. (2018). Phenomenology as a healthcare research method. Evidence Based Journals, 21 , 96–98. https://doi.org/10.1136/eb-2018-102990
Oren, R., Orkibi, H., Elefant, C., & Salomon-Gimmon, M. (2019). Arts-based psychiatric rehabilitation programs in the community: Perceptions of healthcare professionals. Psychiatric Rehabilitation Journal, 42 , 41–47. https://doi.org/10.1037/prj0000325
Shipman, S. D. (2015). The role of self-awareness in developing global competence: A qualitative multi-case study. Graduate Theses, Dissertations, and Capstone s. Paper 21.
Uslu-Ak, B. (2021) Mental health and psychosocial support in Turkey: Practıces, policies and recommendations. Turkish Journal of Social Work Research , 5 (1), 46–55.
Sardogan, C., & Gultekin, B. K. (2023). The frequency of regular participation in the Community Mental Health Center (CMHC) programme of patients with the diagnosis of psychotic disorders and evaluation of related factors. Turkish Journal Clinical Psychiatry, 26 , 264–271.
Sahin, Ş, Elboga, G., & Altindag, A. (2020). The effects of the frequency of participation to the community mental health center on insight, treatment adherence and functionality. The Journal of Clinical Psychiatry, 23 , 64–71. https://doi.org/10.5505/kpd.2020.49369
Soygur, H. (2016). Community mental health services: Quo vadis? Noropsikiyatri Arsivi, 53 (1), 1–3. https://doi.org/10.5152/npa.2016.15022016
Tong, A., Sainsbury, P., & Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care, 19 (6), 349–357. https://doi.org/10.1093/intqhc/mzm042
Townley, G., Brusilovskiy, E., Klein, L., McCormick, B., Snethen, G., & Salzer, M. S. (2022). Community mental health center visits and community mobility of people with serious mental ıllnesses: A facilitator or constraint? Community Mental Health Journal, 58 (3), 420–428. https://doi.org/10.1007/s10597-021-00821-w
Yanos, P., DeLuca, J., Roe, D., & Lysaker, P. (2020). The impact of illness identity on recovery from severe mental illness: A review of the evidence. Psychiatry Research , 288. https://doi.org/10.1016/j.psychres.2020.112950
Yildirim, A., HacıhasanogluAsılar, R., Camcıoglu, T. H., Erdiman, S., & Karaagaç, E. (2015). Effect of psychosocial skills training on disease symptoms, insight, internalized stigmatization, and social functioning in patients with schizophrenia. Rehabilitation Nursing: The Official Journal of the Association of Rehabilitation Nurses, 40 (6), 341–348. https://doi.org/10.1002/rnj.195
Yildiz M. (2011). Psychological social skills training for schizophrenia patients . Turkish Social Psychiatry Association.
Yildiz, M., Kiras, F., Incedere, A., Esen, D., Gurcan, M. B., Abut, F. B., Ipci, K., & Tural, U. (2018). Development of social functioning assessment scale for people with schizophrenia: Validity and reliability study. Anatolıan Journal of Psychıatry, 19 , 29–38. https://doi.org/10.5455/apd.2374
Yildiz, M. (2019). Psychosocial skills training trainer's manual . Umuttepe Publications, 2nd Edition.
Yıldız, M. (2021). Psychosocial rehabilitation interventions in the treatment of schizophrenia and bipolar disorder. Archives of Neuropsychiatry, 58 (Suppl 1), 77–82.
Download references
Acknowledgements
The authors express gratitude to the staff of the mental health center for their support and assistance during the study, as well as to the participants who generously provided responses to the questions posed.
No funding was received for this study.
Author information
Authors and affiliations.
Samsun Mental Health and Diseases Hospital, Samsun, Türkiye
Halil İbrahim Bilkay
Psychiatric Nursing Department, Tokat Gaziosmanpasa University, Tokat, Türkiye
Burak Şirin & Nermin Gürhan
You can also search for this author in PubMed Google Scholar
Contributions
All authors contributed to the study conception and design.
Material preparation, data collection and analysis were performed by Halil İbrahim BİLKAY and Burak ŞİRİN. The first draft of the manuscript was written by Halil İbrahim BİLKAY and all authors commented on previous versions of the manuscript. Nermin GÜRHAN read and approved the final manuscript.
Corresponding author
Correspondence to Halil İbrahim Bilkay .
Ethics declarations
Conflict of interest.
There are no conflicts of interest.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
"The study's abstract was presented as an oral presentation at the 7th International 11th National Psychiatric Nursing Congress (18-20 October 2023) in Ankara".
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Bilkay, H.İ., Şirin, B. & Gürhan, N. Effectiveness of Psychosocial Skills Training and Community Mental Health Services: A Qualitative Research. Community Ment Health J (2024). https://doi.org/10.1007/s10597-024-01278-3
Download citation
Received : 29 January 2024
Accepted : 31 March 2024
Published : 22 April 2024
DOI : https://doi.org/10.1007/s10597-024-01278-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Community mental health center
- Psychosocial skills training
- Qualitative research
- Functionality
- Find a journal
- Publish with us
- Track your research
- Open access
- Published: 24 April 2024
Exploring information needs among family caregivers of children with intellectual disability in a rural area of South Africa: a qualitative study
- Mantji Juliah Modula 1 &
- Mpho Grace Chipu 1
BMC Public Health volume 24 , Article number: 1139 ( 2024 ) Cite this article
Metrics details
Globally, families experience challenges caring for and raising children with intellectual disability (ID). Family caregivers in rural states are mostly known for lacking support resources, including information on understanding the care of ID. Lack of adequate information on understanding of ID compromises the provision of life-long care and support of the children with ID’s physical, emotional, psychological and social developmental well-being. The study aimed to explore the information needs of family caregivers regarding the care of children with ID in rural areas of Limpopo Province, South Africa.
This qualitative explorative research conducted 16 in-depth individual interviews and one focus group discussion with ten family members. The participants shared their experiences of raising children with ID in rural communities. Inductive thematic analysis using Atlas Ti software categorised emerging themes and subthemes of this study from merged data sets on information needs regarding the care of children with ID among family caregivers.
The findings highlighted the need for information regarding ID care among family caregivers raising children with ID in the home environment. The information challenges experienced by family caregivers include caring for the challenging behaviour of children with ID and available support resources and services for the children and their families. These challenges impact the care and support required to meet the developmental needs of children with ID. Furthermore, inadequate information on ID among family caregivers in rural communities with a lack of resources restricts the children from accessing required support services.
Conclusions
Given the information challenges these families face on ID, the stakeholders must develop continuous training programmes that will equip, empower, and further monitor ID care and management among family caregivers to enhance care and the raising of children with dignity.
Peer Review reports
Intellectual disability (ID) diagnosis requires families as primary caregivers to support their children during the developmental stages of life. ID as a neurodevelopmental disorder limits intellectual functioning and adaptive behaviour during the developmental period of a child [ 1 ]. ID ranges from mild, moderate, severe and profound impairment. The diagnosis affects the child’s communication, cognitive and self-care skills development, leading to dependency support living [ 2 ]. Children with ID are prone to physical conditions, including obesity and constipation, often exposing them to misdiagnosis and underdiagnosis [ 3 ], limiting their access to healthcare services. Early diagnosis of ID enables early intervention and enhances acceptance of the child by the community [ 4 ].
Globally, ID affects approximately 2–3% of the general population [ 5 ], and the prevalence of children under five is 3.2% [ 6 ]. The incidence in low-income countries is 16.41/1000; in middle-income countries, it is 15.94/1000 persons, higher than in other countries, with approximately 9.21/1000 persons [ 4 ]. South Africa experiences a lack of data on the prevalence of ID and is further dependent on the census.
ID diagnosis generally increases the lifelong dependency of the children on their families regarding self-care and support to thrive. As a primary caregiver, every family is an environment where essential interpersonal experiences of a child’s development occur [ 7 ], including personality, behaviour, and attitudes. Even though families take the lead in raising these children, ID awareness and information among the carers has been a continued concern [ 8 ]. In addition, information created for childrearing may not benefit caregivers of children with ID [ 9 ]. In most cases, families of children with ID experience parenteral barriers, including limited knowledge related to a lack of resources or support [ 10 ].
Past research established that children with ID are more at risk of experiencing childhood problems than their peers without ID [ 11 ]. As most children with ID have a prevalence of developmental delay impacting their independence ability [ 12 ], their care requires information and understanding of ID. Past research has shown that adequate knowledge is measured through the caregiver’s confidence in a particular realm or topic to declare the knowing of what, how, when and why questions that inform one’s attitudes and further influence one’s behavioural changes [ 13 ].
Quality caregiving of a child with ID influences their developmental outcomes [ 14 ]. It is noteworthy that parents’ understanding of the capacity to care for children with ID is assessed based on their responses to the needs of such children [ 15 ]. Previous studies highlighted how the families were more reactive than proactive regarding caring for their children with ID, leading to social exclusion by their communities [ 16 ]. Although the need for training of parents raising children with ID has broadly been investigated successfully [ 17 ], exploring information needs on the care of ID among primary caregivers in rural areas has yet to be fully established.
South Africa surpassed an estimated population of 60 million, with more than 19 million people residing in rural jurisdictions. The country still needs improvement in service delivery problems, especially in rural states. The pastoral population’s life challenges are unique and mainly complex due to geographical and race/ethnicity characteristics [ 18 ]. Previous studies on the experiences of families of children with ID in the South African rural context revealed challenges related to poverty, poor education, and unemployment, including limited transport to access professional services and support systems for ID [ 19 , 20 , 21 , 22 ]. Furthermore, rural communities report low access to health services, including a scarcity of professionals and specialist care, exposing them to health risks resulting in shorter life expectancy [ 23 , 24 ].
Evidence from previous research established that the diagnosis of children with ID in rural areas is likely delayed due to geographic barriers to access services, causing health disparity for children compared to their peers in urban areas [ 25 ]. This delay prevents families from receiving information relevant to planning and managing the child’s care, which is considered a way of simplifying the processes of the professionals [ 26 ]. The family caregivers of children with ID require information including health specialists and rehabilitation services for their children, government support grants, networking and educational services [ 27 , 28 ]. The social model posits that the lack of information access experienced by caregivers of children with ID limits their parenting abilities and further impacts the support of the functioning level of their children [ 29 ]. The study aimed to explore the family caregivers’ information needs regarding understanding the care of children with ID in rural areas to fill the gaps in the caring and management challenges of ID in the home environment. Adequate information by families regarding the care of ID is vital in meeting the support needs of their children with ID in rural areas. These require comprehensive care, support, and rehabilitation for children and their families. The study’s objective was to explore and describe the information needs of family caregivers regarding the care of children with ID in rural areas of Limpopo Province, South Africa.
Study design
This qualitative explorative research helped the researcher facilitate data collection, analysis, and interpretation of the finding processes [ 30 ]. The approach enabled an unrestrained process that explored the participants’ information needs regarding the care of children with ID in a rural home environment. The focus group discussion and in-depth individual interviews allowed participants to share their experiences caring for and managing a child with ID in a rural community. The first researcher recruited participants, collected data, analysed, and wrote manuscripts. The second author reviewed the manuscript.
The researcher conducted the study in the Capricorn district municipality of Limpopo Province, which is approximately 80% rural and estimated at 5.8. million population [ 31 ]. The district is one of the five municipalities of the province and has a growing economic centre. It is known for providing better community services such as job opportunities, schooling, and health care facilities in the province. Thus, it attracts a high population density with a unique cultural heritage, diverse ethnicities, and five languages under 30 traditional authorities [ 31 , 32 ]. The district’s households in the rural community experience challenges regarding limited access to basic needs, including piped water, poor hygienic sanitation conditions and restricted access to health and education services. The high unemployment in this rural status contributed towards people migrating to other provinces for job opportunities, leaving most families to female and single-headed households [ 33 ].
Participants and sampling
The study sampled 26 families from different tribal authorities of Capricorn district with the core function of directly caring for and raising children with ID in home environments. The vulnerability of family caregivers resulted in some hiding their children from their communities due to social stigma related to ID diagnosis. The researcher recruited participants whose children were accessing education and health facilities in their communities through purposive and snowballing sampling strategies. The strategies assisted the researcher in reaching those families not known to community facilities, including schools and health care services, as their children were not utilising such services. The family caregivers recruited, invited, and introduced other families who were relatives or neighbours or encountered them at churches or community meetings and met inclusion criteria to the researcher [ 30 ]. Such families’ children were diagnosed with ID from hospitals in other provinces and private health care services. They did not use public services, fearing discrimination related to stigmatisation from their communities.
Eligibility criteria included any family caregiver above 18 years who was living and directly involved with raising children with ID and was voluntarily willing to share their experiences regarding caregiving informational needs in the rural home environment. Furthermore, the researcher’s judgement stayed instrumental in the selection of family caregivers whose children were of school-going age or over six years old, indicating that they were not recently diagnosed with ID. For most children at this age, healthcare professionals have already established their diagnosis of ID, as their developmental capabilities were able to be assessed with their peers at school. Furthermore, on this ground, the researcher’s opinion assumed that children were emotionally ready to express their feelings in their life circumstances. The researcher further believed such participants had adequate information to relate their experiences as primary family caregivers raising children with ID. The researcher excluded family caregivers of children with IDs less than 6 and above 19 years old and those family members who did not live with the children in a home environment.
The family caregivers were between 19 and 67 years old, and most left schooling at the secondary level. The sample comprised 16 mothers, one father, two grandparents (one grandfather and one grandmother), three aunts, two uncles and two guardians of the children with ID. Table 1 below indicates the participants’ demographic information and the profile of children with ID.
Most participants were females, 85%, showing that caring for children with ID was on their shoulders. Most men migrated to cities looking for jobs. Half of the participants left schooling before Grade 12, while few obtained tertiary qualifications. Participants indicated a need for more funds as a contributory factor for not proceeding to tertiary education. Most participants were unemployed at 61%. The interview guides helped the researcher to profile information about the children, including age, gender, and other health problems. In addition, the researcher asked participants for more details of medical treatment for those experiencing other health problems besides ID diagnosis. Participants reported their children with ID experiencing comorbidity problems, including speech and hearing, dental and epilepsy, requiring health care support. Female-headed households were at 38%, and single parents at 42%. Most children were males with fewer father figures. The ages of the children were between 6 and 17 years and mostly experienced speech problems at 37% and unattended dental issues, including missing teeth and tooth decay at 30%, requiring health care services. The dental problems were mainly related to the difficulty of the children with ID to identify and report their needs to their caregivers compared to their peers without ID.
Data collection
The researcher conducted 16 in-depth interviews followed by one focus group discussion of 10 family members raising children with ID in a home environment. The individual in-depth interviews enabled the asking of predetermined questions and focus group discussion triangulation to enhance the richness of data. The participants shared their experiences of caring for their children with ID in a rural environment with the first author. All family caregivers signed written consent to participate before the commencement of data collection. Observational field notes complemented capturing pertinent data not documented through the audio recorder, including the participants’ emotional expressions towards answering questions. Participants gave verbal consent for their narratives to be audio-recorded. The researcher maintained the anonymity and confidentiality of participants throughout the data collection process to protect their human dignity.
Semi-structured interview guides directed the interviews and focus group discussion to explore family caregivers’ experiences raising children with ID in rural communities. The researcher used professional assistance in translating interview guides into the Sepedi language, which is dominant in the district and understood by participants. The researcher was fluent in languages preferred by the participants. The interview guides for in-depth interviews and focus group discussion collected socio-demographic information under section A. The central question was asked about the experiences of raising a child with an intellectual disability, followed by probing questions. The guides enabled comparability amongst data sets of focus group discussions and in-depth individual interviews.
Data analysis
The researcher analysed data concurrently with the collection process. The inductive thematic data analysis with the assistance of the Atlas Ti software program followed qualitative analysis steps (Rubin & Rubin, 2012) [ 34 ] of familiarising oneself with data, generating initial codes, searching emerging themes, reviewing them, and naming their related and subthemes. Data analysis consolidated individual in-depth interviews and focus group discussion data. The first researcher (MJM) translated data into English and transcribed audio-recorded information from both data sets on an Excel Sheet. The researcher read written transcripts with written observational field notes to acquaint oneself with the collected data. The observational field notes maximised analysis in documenting participants’ emotional and psychological status attached to their narratives, further increasing reliability and validity. The researcher allocated various codes to participants according to associated themes. The researcher removed any information linking participants to data to ensure anonymity and confidentiality. Transcripts were loaded to Atlas Ti software to arrange similar codes using the coding manager. The Atlas Ti assisted the researcher in handling multiple overlapping codes without losing their contexts. The researcher conducted content analysis to determine themes and subcategories from frequently occurring styles and patterns in the participants’ narrative statements. Data from both participant groups were duly categorised and compared, including examination of any connections, regularities, variations and peculiarities. The researcher summarised information into meaningful units, presented in thick descriptions and quotes from the participants to demonstrate their authenticated voice in the context of supporting literature-based evidence [ 35 ]. The academic supervisor of the study confirmed the appropriateness of the findings.
The researcher comparably consolidated data analysed from 16 in-depth individual interviews and one focus group discussion of 10 female family caregivers raising children with ID. Table 1 presents the profiles of participants and their children with ID. The results revealed information needs regarding the care of children with ID among family caregivers in rural areas. Most families showed a quest for information regarding the care of children’s challenging behaviour and available resources to enable the caregiving of children with ID. The researcher allocated participants’ narrative numbers, such as Participant 1, age, relationship to the child and the type of interviews, to ensure their anonymity and confidentiality throughout the study. Table 2 presents the generated themes and subcategories of the results.
Caregiving of challenging behaviour of children with ID
This theme emerged during focus group discussion around their experiences of the challenging behaviour of children with ID. In addition, the in-depth individual interview responses on supporting families raising children with ID highlighted that most children display challenging behaviour, and most participants reported difficulties in handling them. Participants communicated the theme as a way to make sure that their children were always safe. The results showed the need for information to understand the care of their children’s challenging behaviour. Family caregivers needed information regarding impaired social interaction of the child, overprotectiveness and caretaking attachment toward their children with ID. The diagnosis of ID limits the intellectual adaptive behaviour of children with ID, including impaired social and emotional well-being that resulted in some family caregivers being overprotective and developing a caretaking attachment to approach and cope with the care of their children.
Impaired social interaction of the child
Some participants were concerned about their children’s poor social interaction challenges within and outside the home environments. Most children reported being more comfortable staying at home with familiar family members. The families found introducing these children to new faces, including their peers, difficult.
“My child doesn’t want to meet people outside the family members. He is more comfortable to stay home” (Participant 5, mother, 63 years, focus group). “ My child is having a problem refusing to be sent to the shop near home to buy bread, and he will tell you to send his younger sibling. We cannot force him ”. (Participant 16, mother, 54 years). “My child doesn’t want to go anywhere. He stays at home. He does not want to visit anywhere, even his sister. I even left him alone at home now” (Participant 12, mother, 43 years, individual interview).
Some families needed more information to understand that intervening in children’s behaviour can improve with regular medical help provided by professionals. However, some participants found it challenging to associate refusing to be sent or going anywhere outside the home with impaired social interaction, where the child experiences challenges meeting unfamiliar faces. In addition, participants believed that the children decide to stick to the family environment, including disobedience. In other instances, rejection by community members related to stigma can result in poor interaction of the children with ID with other community members outside the home.
Impaired emotional well-being of the child
The families highlighted the information to deal with different emotions and mood disorders displayed by their children with ID. Some participants indicated emotional dysregulation among the children with ID, contributing to their stress levels as family caregivers. Speech problems experienced by children with ID resulted in most children not being able to express their needs, thus leading them to display challenging behaviour, such as crying for attention.
“The child does not want to stay alone, but she needs attention. She will cry even when nothing is happening to her. I mean like crying unexpectedly. I need training on how to treat her properly” (Participant 23, father, 55 years, individual interview) . “I need more information on how to take care of the child. Especially to manage her when she is angry because of her strange behaviour. I will be happy if they can teach me so I don’t stress too much” (Participant 9, aunt, 42 years, focus group).
Participants believed that adequate information on the care of children with ID would help control and manage their children’s challenging behaviour. These will further reduce the caregiver’s stress level and increase their caregiving skills and self-efficacy towards the difficulties related to the conduct of their children with ID.
Overprotectiveness towards the child
Some families displayed and reported an overly protective approach towards their children with ID. Family caregivers gave individual attention to children more than other children at home. The families were concerned that their children with ID need more protection as they cannot stand for themselves. Participants showed the need for information to be able to treat their children equally.
“I must pay attention and listen to the child more than anyone in the family because he is not able to take care of himself.” (Participant 11, guardian, 27 years, individual interview). “I have other children besides him. I don’t have time for other children; I think I give more attention to him only; I need training to know how to treat other children because this causes conflict”. (Participant 1, mother, 44 years, focus group).
The delayed development of ID in self-care of the children resulted in dependency of the children on the care and support of family caregivers. However, some families felt that the children should not be treated like other children and care for the children more than their siblings. These could further contribute to the rejection of the child by siblings. Social stigma and lack of inclusiveness of the children with ID could contribute to the family caregivers feeling responsible for protecting their vulnerable children more than any other children. Thus, there is a dire need for information to enable family caregivers to provide care of children with ID without feeling guilty and neglecting the parental care of other children.
Caretaking attachment towards the child
Some families reported that children were close to their family members and felt more comfortable around their mothers as caregivers. However, some family members found it difficult to share the caretaking responsibility of the children with other persons willing to help.
“He refuses to sleep with his siblings. He cries to share a bed with me, and it is not easy because I am married” (Participant 13, mother, 35 years, individual interview). “I do not believe in taking the child to institutions like boarding. I think that the child will think that I don’t like him and have abandoned him” (Participant 16, mother, 54 years, individual interview).
Family caregivers communicated caretaking attachment to ensure that children receive full support related to their dependency on the family members’ care. Some felt responsible for providing care independently and needed more trust in other facilities with trained professionals to care for and manage their children with ID. Both children and family caregivers found it difficult to wean from caretaking attachment. However, some responses indicate that caring for a child with ID could bring intense bonding, impacting the family’s quality of life. These narratives highlight the need for professional family interventions.
Available child and family support services
The researcher generated this theme from both focus group discussions and in-depth individual interviews on responses around the available resources to care for and support the families caring for and raising children with ID. The results showed that family caregivers need information on services available for their support as primary caregivers and their children with ID. Support services enable caregivers raising children with ID to cope with the challenges and burdens of care.
Counselling services
This study found that most families needed information to access critical health and well-being services involving counselling as professional assistance in public institutions, which is provided free to such families. Some participants reported an inability to cope with the stress of meeting the needs of their children with ID, especially single parents who experienced difficulties meeting their children’s needs. However, they needed the information to access such support services.
One mother who separated from her husband displayed a dire need for counselling services to deal with caring challenges. Her narrative and observational field notes highlighted the frustration of dealing with her child’s care without her partner’s support. The result communicates the need for continuous counselling to enable ongoing support of parenting skills needed to care for the child with ID in a home environment.
“I was not coping and needed counselling for this matter. But did not know where to go for help.” (Participant 21, mother, 32 years, individual interview).
Some participants reported difficulties in dealing with the fact that their children were diagnosed with ID. The narratives indicate the information needed for counselling services to enable coping abilities.
“I just accepted, but at the beginning, I was not coping. I always take whatever is happening and take it very lightly. I still have unanswered questions. It is difficult to let it go” (Participant 10, mother, 45 years, focus group). “I am not sure of the services [counselling] provided to such families; what I know is that we do not have services for the children” (Participant 11, guardian, 27 years, individual interview).
Some participants believed that information on counselling services would enable them to access professional support for reducing stress levels and using adaptive coping mechanisms to deal with caring responsibilities. Mothers of children with ID mostly communicated the need for counselling services.
Social work services
The family caregivers needed access to information to understand the social workers’ services as a support system for their children’s needs. Some used these services for other family problems but less for raising children with ID. They needed information on collaborations between themselves and the social workers to support and provide care to their children with ID.
“ I consulted the social worker in 2012 when we had family issues. The social workers have never visited my child. I even asked them to visit my house, but they never came” (Participant 14, mother, 42 years, individual interview). “ We once decided to apply for him to be institutionalised but did not succeed ” (P articipant 25, uncle, 31 years, individual interview).
Some families were willing to institutionalise their children with ID for different reasons. However, they needed more information on the processes to follow. In most cases, such an institutionalisation process in South Africa is coordinated and finalised through social work services. The communicated evidence further showed the need for home visits by health professionals that will improve individualised family interventions on the information needed for the child’s care. Socio-demographic information revealed that most participants utilised the social work services when making applications for the children’s dependency grants but needed help to continue with the services for information regarding further assistance in the care of such children.
Psychological services
Some families were not coping with the diagnosis of their children with ID. The burden experienced by these families leads to some willing to end their lives to deal with the impact of raising a child with ID. One single mother of 5 children was emotional when sharing her experiences:
“I was frustrated and wanted to ingest poison and kill both my children. I felt the pain” (Participant 14, mother, 42 years, individual interview). “I feel emotional pain that he is like the way he is, not the same as other children” (Participant 18, mother, 50 years, individual interview).
The excerpts above show evidence of hopelessness related to the burden of raising a child with ID. The care burdens required psychological intervention services to assist the needy family caregivers. The observations on these parents displayed signs of emotional and psychological drains of raising a child with ID. The diagnosis of children with ID showed frustration, especially among mothers who experienced emotional and psychological impacts.
Health care services for children with ID
Most children experienced health-related challenges that required intervention in health services such as medical, dental, speech and hearing, and mental health services. Some families needed to utilise community facilities such as clinics to support their children’s basic needs with ID effectively. However, few participants reported taking their children to health care services. Stigmatisation resulted in some family caregivers not being at ease in seeking help to bring their children to health care professionals. However, services for such children are provided freely in South African public institutions.
“My child shuffles on the floor and cannot walk or sit. I took him [the child] to the church to receive healing. I think mental problems get different treatment from other diseases. I don’t know the services around us to help my child.” (Participant 20, mother, 47 years, individual interview). “I sometimes fail to understand what he wants, especially around people. I get frustrated because I do not understand the sign language that he is using. It is challenging to understand him. (Participant 1, mother, 44 years, focus group). “She lost most of her teeth, and it was difficult to save them. They started by decaying, and most of the time, she refused to chew hard food, complaining of pain. I didn’t take her to the hospital as the tooth fell without anyone removing it. Now, she eats eggs” (Participant 19, mother, 36 years, individual interview). “I wake up during the night when he is fitting. I can hear him struggling when I am asleep. I must make sure that everything is right with him. The child is not on treatment.” (Participant 6, mother, 42 years, focus group).
The evidence shows that some family caregivers needed information to understand the communication displayed by children with speech problems to respond to their basic needs. Such children require caregivers’ knowledge of primary sign language to facilitate training and rehabilitation of their developmental needs. Lack of adequate information on ID resulted in some families finding alternatives for medical care, such as spiritual and traditional care, for assistance with their children’s health challenges with ID. The dental problems comprised the nutrition of the children as they could not eat hard food, exposing the children to malnutrition.
The results evidenced that although South Africa provides free healthcare services to all citizens at primary healthcare facilities, access to specialised professionals still needs to be improved. Most children experienced health challenges, including epilepsy, physical impairment, speech and hearing problems and dental issues requiring special attention. The study indicates that disseminating information on available ID resources will empower families to provide needed care to their children.
Discussions
The study explored the information needs of family caregivers regarding the care of children with ID in rural home environments. The results established that most families as primary caregivers experienced information challenges regarding caring for their children’s challenging behaviour and the available support resources in their communities. Furthermore, the need for more information on social support structures in rural areas environment regarding the care and raising of children with ID restrains the inclusiveness of these children to participate in societal activities [ 36 ].
Family caregivers needed information to understand and handle challenging behaviour and grooming of their children to possible independence. In support, past research found that parents seek information on the care of their children with ID from professionals to cope with the burden [ 37 ]. On the other hand, research revealed that the knowledge of families of children on ID mostly depends on the type of information provided by the professionals educating them [ 38 ]. In line with the findings, the previous research found a lack of dissemination to family caregivers of children with disabilities in welfare information by the Indian government [ 39 ]. The results extend to prior studies that found information increasing, knowledge and understanding of the parents’ level of children with ID, further leading to self-advocacy in proactive decision-making on the care [ 40 ].
Previous research that resonates with this study found that knowledge is good if shared with caregivers who require it to meet the children’s developmental needs [ 41 ]. However, the empowerment of families of children with ID is mainly determined by their economic status and educational level [ 42 , 43 ]. In support, previous results indicate that the caregivers’ awareness of ID is allied to resilience ability, which mainly enhances the care of children with ID [ 44 ].
This study is congruent with the reflection that reported that caregivers found the behavioural needs of their children with ID challenging to fit into other environments and required expertise to handle them [ 45 ]. Behavioural challenges in ID may indicate the children need attention regarding stimulation, pain reduction, social escape and tangible reinforcement [ 46 ]. Some children presented with impaired social interaction with other family and community members. Similarly, it was revealed that children with ID have few interactions with other people and experience rejection or isolation [ 47 ]. This finding supports the study established that the environmental and social enablers, including inclusivity in activities by their communities, can determine the children’s social interaction [ 48 ]. Congruent with these findings, previous results found that information given to the family caregivers on the children’s behaviour, including emotional changes and aggression, improved their skills to handle the child and further increased feelings of competence and confidence [ 49 ].
Most family caregivers resorted to coping mechanisms that involve caretaking attachment and overprotective towards their children with ID. This finding resonates with the research that found that parents with less information on ID were inadequately involved in modelling behaviour that was adaptive to the development of their children with ID [ 50 ]. The study results support the finding that Australian children with ID experience emotional and behavioural problems challenging to their caregivers [ 51 ]. In addition, the conclusions aligned with the study, which found that in Spain, parents felt responsible for the happiness of their children and developed an overprotective approach towards their care [ 52 ]. Comparably, a caretaking attachment bond mainly develops between the child and caregiver based on love, interaction, and the child’s feeling more uncomfortable in the caregiver’s absence [ 53 ]. Hence, the overprotectiveness of children with ID sometimes makes it difficult for caregivers to combine their work life and the care of their children with ID [ 52 ]. However, a similar study revealed that households with extended family members share the care responsibilities for children with ID, reducing the caring burden [ 54 ].
The study highlighted the need for information to empower the family caregivers on the services available in the communities to offer them support, including counselling, social work, psychological care, and health care services for their children. The findings further resonate with the study, which reported that the caregivers of children with ID needed to be made aware of the support resources available to their health needs [ 25 ]. Most families with children with ID are highly vulnerable and require support interventions for their well-being [ 39 ]. This study highlights that family caregivers, primarily mothers, need information on counselling services to cope with the care challenges of raising their children with ID. In support of this finding, a study conducted in South Africa indicates that most children with developmental disorders were under the care of mothers who are primary caregivers [ 55 ]. Similar research established that counselling of families of children with ID decreases their stress levels, increases their self-esteem and further reduces the risk of disorders related to anxiety [ 56 ]. Furthermore, congruent with these findings, a study revealed that counselling was crucial in enabling family members to create a friendly, positive home environment for their children with ID [ 57 ].
The information needed for health care services included medical, dental, and speech challenges experienced by the children with ID. Some family caregivers reported their children presenting with dental problems such as loose and missing teeth. Comparable studies found that caregivers could identify the dental pain of their children with ID through salivation and putting hands in their mouths more often than their typical peers [ 58 ]. In addition, congruent with this finding, the speech of children with ID is more emotional and requires stimulation than their typical development peers [ 59 ]. In alignment with this finding, accessing appropriate professional services in rural Australia was challenging due to geographical distances [ 60 ]. In support, the study in South Africa revealed that public facilities experience a long list of bookings [ 61 , 62 ]. These reduce access to available rural support services and resources to cater for the needs of the children with ID and their families.
Suggestions and recommendations for practice
The study recommends prioritising the information needs of children with ID and their families to receive professional assistance. Policymakers should establish, support, and provide resources on awareness of ID within health and education facilities. Furthermore, the development of directive policies and regulations should strengthen the implementation of education and training programmes on ID awareness within societies. Collaboration of health care professionals and essential service providers, including teachers and educators in early childhood development centres and schools, should support the dissemination of information on ID to the public. In addition, the results recommend ID awareness campaigns and community education regarding the care of children with ID and the support of caregivers. Thus, training nurses, midwives, social workers, and other health professionals, including educators, is vital to enable them to provide ID awareness and train family caregivers. Training of available community healthcare workers and traditional and religious leaders on ID will equip them with the knowledge to be able to support the vulnerable family caregivers of children with ID. These will provide the families with continuous, valuable, updated information to help their children.
Furthermore, the study highly recommends collaborative professionals for training, empowerment, and providing psychoeducational interventions that will strengthen caregiver competence and confidence in ensuring continuity of the caregiving of children with ID from the home environments. Collaboration and coordination of educational facilities, social development, rehabilitation, and health care services will further enhance information on ID for the public. The study suggests that professionals should actively facilitate forming community support groups and home-based care services to interact and equip family caregivers with relevant information regarding ID awareness to reduce social stigma. Forming partnerships with family caregivers will strengthen information giving and access.
The study’s limitations involve data on the prevalence of children with ID in Limpopo Province that were not available. The study could not capture the experiences of family caregivers of children with ID not accessed through snowballing and known to community health care facilities. Fathers of the children with ID were less presented, limiting their narrative experiences on the caregiving of their children. The study has no information on professional facilities available for support services in rural communities.
This study provides insights into the information access and understanding of family caregivers of children with ID in rural areas of Limpopo Province. The study findings indicate the need for information access by these families to understand the care of their children with ID. The study shows the crucial responsibility of service providers to activate the information support system of caregivers raising children with ID in rural home environments. The findings of this research hope to inform the establishment of training programmes to improve ID information by empowering and enabling family caregivers in rural areas to improve understanding of the care of their children with ID. Training programmes that continuously update caregivers’ knowledge of ID play a critical role in enhancing self-efficacy and competency to support their children. The study supports stakeholders’ collaboration on ID awareness campaigns and opens more platforms to disseminate information and educate the public, including those in rural areas with fewer resources.
Data availability
The datasets used and analysed during the current study are available from the corresponding author upon reasonable request. The data are not publicly available due to information that could compromise the privacy of the research participants. Please write to [email protected].
Abbreviations
- Intellectual disability
American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM -5™. 5th ed. Library of Congress; 2013.
Arnett AB, Wang T, Eichler EE, Bernier RA. Reflections on the genetics-first approach to advancements in molecular genetics and neurobiological research on neurodevelopmental disorders. J Neurodev Disord. 2021;13:24. https://doi.org/10.1186/s11689-021-09371-4 .
Article PubMed PubMed Central Google Scholar
Liao P, Vajdic C, Trollor J, Reppermund S. Prevalence and incidence of physical health conditions in people with intellectual disability– a systematic review. PLoS ONE. 2021. https://doi.org/10.1371/journal.pone.0256294 . 16,8,e025629.
Elmasry HMA, Aladawy MA, Abd-elhamid MM. Prevalence and Risk Factors of Intellectual Disabilities in Children. EJHM . 81, 1, 1307–1313. http://creativecommons.org/licenses/by/4.0/ (2020).
S´anchez-Luquez KY, Carpena MX, Karam SM, Tovo-Rodrigues L. The contribution of whole-exome sequencing to intellectual disability diagnosis and knowledge of underlying molecular mechanisms: a systematic review and meta-analysis. Mutat Res Rev Mutat Res. 2022. https://doi.org/10.1016/j.mrrev.2022.108428 .
Article PubMed Google Scholar
Olusanya BO, Kancherla V, Shaheen A, Ogbo FADAC. Global and regional prevalence of disabilities among children and adolescents: analysis of findings from global health databases. Front Public Health. 2022. https://doi.org/10.3389/fpubh.2022.977453 .
Agai A, Zhekov Z. Attitudes of the parents with different status (parent/guardian) regarding the competences of the adults with intellectual disability to independent living. Int J Knowl. 2019. https://doi.org/10.35120/kij31061839a . 31,6,1849– 1844.
Article Google Scholar
Ahmad W, Nazli, Chavan BS. Knowledge, attitude, and practice among parents about sex education of their children with intellectual disability. Indian J Soc Psychiatry. 2022. https://doi.org/10.4103/ijsp.ijsp29720 . 38,357– 61.
Machalicek W, Lang R, Raulston TJ. Training parents of children with intellectual disabilities: Trends, Issues, and future directions. Curr Dev Disord Rep. 2015;110–8. https://doi.org/10.1007/s40474-015-0048-4 .
Sapiets SJ, Hastings RP, Stanford C, Totsika V. Families’ Access to early intervention and supports for children with Developmental Disabilities. J Early Interv. 2023;45,2:103–21. https://doi.org/10.1177/10538151221083984 .
Fauth RC, Platt L, Parsons S. The development of behavior problems among disabled and non-disabled children in England. JADP. 2017;52:46–58. http://eprints.lse.ac.uk/82634 .
Murphy R, et al. Estimated prevalence of disability and developmental delay among preschool children in rural Malawi: findings from Tikule Limodzi, a cross-sectional survey. Child Care Health Dev. 2020;46:187–94. https://doi.org/10.1111/cch.12741 .
Schrader PG, Lawless KA. The knowledge, attitudes, & behaviors Approach: how to evaluate performance and learning in Complex environments. Perform Improv. 2004;43:9. https://doi.org/10.1002/pfi.4140430905 .
Vilaseca R, Rivero M, Leiva D, Ferrer F. Mothers’ and fathers’ parenting and other family context variables linked to developmental outcomes in young children with intellectual disability: a two–wave longitudinal study. J Dev Phys Disabil. 2023;35:387–416. https://doi.org/10.1007/s10882-022-09856-7 .
Norlin J, Randell E. Social workers’ perceptions of assessing the parental capacity of parents with intellectual disabilities in child protection investigations. J IntellectDisabil. 2022;0:0,1–18. https://doi.org/10.1177/17446295221113717jid .
Ericson S, Stadskleiv K, Hesla MW. Gaining super control: psychoeducational group intervention for adolescents with mild intellectual disability and their parents. J Intellect Disabil. 2022;6,2:350–64. https://doi.org/10.1177/1744629521995373 .
Mohamed AR, Sterkenburg P, Van Rensburg E, Schuengel C. Adapting attachment and Biobehavioral catch-up for infants and young children with intellectual disabilities and developmental delays in South Africa: reflections and recommendations from local stakeholders. Infant Ment Health J. 2022;1–22. https://doi.org/10.1002/imhj.22027 .
Leider JP., et al. The State of Rural Public Health: Enduring needs in a New Decade. AJPH Rural Health. 2020;110(9):1274–343. https://doi.org/10.2105/AJPH.2020.305728 .
Cantero-Garlito PA, Flores-Martos JA, Moruno-Miralles P. Care of children with disabilities in rural areas: meanings and impact on everyday life and Health. Study protocol. Int. J Qual Methods. 2020;19:1–7. https://doi.org/10.1177/1609406920947602 .
Chauke T, Poggenpoel M, Myburgh CPH, Ntshingila N. Experiences of parents of an adolescent with intellectual disability in Giyani, Limpopo province. South Africa’ Health SA Gesondheid. 2021. https://doi.org/10.4102/hsag.v26i0.1538 .;26,0, a1538.
Modula MJ. The support needs of families raising children with intellectual disability. Afr J Disabil. 2021;11(0):a952. https://doi.org/10.4102/ajod.v11i0.952 .
Sadiki MC. Parenting a child with disability in rural South Africa: navigating the healthcare system. Afr J Disabil. 2022;11. a942.
Fortney S, Tass’e MJ. Urbanicity, health, and access to services for people with intellectual disability and developmental disabilities. AJIDD 126. 2021 https://doi.org/10.1352/1944-7558-126.6.492 .
Huus K, Dada S, Bornman J, Lygnegård F. The awareness of primary caregivers in South Africa of the human rights of their children with intellectual disabilities. Child: Care Health Dev. 2016;42:863–70. https://doi.org/10.1111/cch.12358 .,6,.
Article CAS PubMed Google Scholar
Singh RL, Moody EJ, Rigles B, Smith EB. What it takes to raise children with autism in a rural state. Adv Neurodev Disord. 2018. https://doi.org/10.1007/s41252-018-0082-4 .
James N. The formal support experiences of family carers of people with an intellectual disability who also display challenging behaviour and mental health issues: what do carers say? J IntellecT Disabil. 2013;17:1,6–23. https://doi.org/10.1177/1744629512472610 .
Sefotho MN, Ferreira R, Lushozi BB. The quest for ongoing support by parents of learners with intellectual disabilities. J Educ. 2021. https://doi.org/10.17159/2520-9868/i85a05 .
Trafford Z. People don’t understand what we go through! Caregiver views on South Africa’s care dependency grant’. Afric J Disabil. 2023;12. 0,a111;.
Koolen J, van Oorsouw W, Verharen L, Embregts P. Support needs of parents with intellectual disabilities: systematic review on the perceptions of parents and professionals. J Intellect Disabil. 2020;24,4:559–83. https://doi.org/10.1177/1744629519829965 .
Saldana J, Omasta M. Qualitative research: Analysing Life. Thousand Oaks: Sage; 2018.
Google Scholar
Capricorn District Municipality. Annual report 2017/2018. http://www.localgoverment.co.za (2017).
South Africa (Republic). Department of Social Development. The White Paper on families. Pretoria: Government Printer; 2013.
Modula MJ, Sumbane GO. Families’ experiences on Safety needs of children with intellectual disability. Int J Environ Res Public Health. 2022;19:15246. https://doi.org/10.3390/ijerph192215246 .
Rubin HJ, Rubin IS. 2012. Qualitative interviewing: The art of hearing data. 3rd edition. Thousand Oaks: Sage.
Henning E, Van Rensburg W, Smit B. 2013. Finding your way in qualitative research. 1st edition. Pretoria: Van Schaik.
Oliver M. The politics of disablement. Macmillan Education; 1990.
Beighton C, Wills J. Are parents identifying positive aspects to parenting their child with an intellectual disability or are they just coping? A qualitative exploration. J Intellect Disabil. 2017;21,4:325–45. https://doi.org/10.1177/1744629516656073 .
Douglas T, Redley B, OttmannG. The need to know: the information needs of parents of infants with an intellectual disability-a qualitative study. J Adv Nurs. 2017;73,11:2600–8. https://doi.org/10.1111/jan.13321 .
Vadivelan K, Sekar P, Sruthi SS, Gopichandran V. Burden of caregivers of children with cerebral palsy: an intersectional analysis of gender, poverty, stigma, and public policy. BMC Public Health. 2020. https://doi.org/10.1186/s12889-020-08808-0 ..20,645.
Jandrić S, Kurtović A. Parenting sense of competence in parents of children with and without intellectual disability. EJOP. 2021;17(2):75–91. https://doi.org/10.5964/ejop.3771 .
Genik LM, McMurtry CM. Reflections and considerations for knowledge translation efforts on pain training for caregivers of children with intellectual and developmental disabilities. ISAP. 2020;22(2):2–24. https://hdl.handle.net/10214/21392 .
Wakimizu R, Fujioka H, Nishigaki K, Matsuzawa A. Family empowerment and associated factors in Japanese families raising a child with severe motor and intellectual disabilities. Int J Nurs Sci. 2018;5:370–6. https://doi.org/10.1016/j.ijnss.2018.09.006 .
Saini R, Ahmad W, Nazli. Awareness among parents of individuals with intellectual disability about sexual health education. Ind Psychiatry J. 2021;30:2,224–9. https://doi.org/10.4103/ipj.ipj7421 .
Jojo N, Nattala P, Seshadri S, Krishnakumar P, Thomas S. Knowledge of sexual abuse and resistance ability among children with intellectual disability. Child Abuse Negl. 2020. https://doi.org/10.1016/j.chiabu.2022.105985 ..136.
Kiernan K, Mitchell D, Stansfield J, Taylor C. Mothers’ perspectives on the lived experience of children with intellectual disability and challenging behaviour. J Intellect Disabil. 2019;23,2:175–89. https://doi.org/10.1177/1744629517737149 .
Medeiros K, Rojahn J, Moore LL, Ingen DJ. Functional properties of behaviour problems depending on level of intellectual disability. J Intellect Disabil Res. 2014;58:2,151–61. https://doi.org/10.1111/jir.12025 .
Vasileiadis I, Maro Doikou-Avlidou M. Enhancing social interaction of pupils with intellectual disabilities with their general education peers: the outcomes of an intervention programme. J Res Special Educational Needs. 2018;0(0). https://doi.org/10.1111/1471-3802.12410 .
World Health Organisation. Towards a Common Language for Functioning, Disability and Health. The International Classification of Functioning, Disability and Health. (Geneva, 2002).
Hewitt O, Keeling N, Pearce M. Training a family in physical interventions as part of a positive behaviour support intervention for challenging behaviour. Br J Learn Disabil. 2016;44,2:159–66. https://doi.org/10.1111/bld.12130 .
Bizzego A, et al. Child disability and caregiving in low and middle income countries: big data approach on open data. Res Dev Disabil. 2020;107:103795. https://doi.org/10.1016/j.ridd.2020.103795 .
Teague SJ, Newman LK, Tonge BJ, Gray KM, The MHYPEDD Team. Attachment and child behaviour and emotional problems in autism spectrum disorder with intellectual disability. J Appl Res Intellect Disabil. 2020;33:475–87. https://doi.org/10.1111/jar.12689 .
Fernández-Ávalos MI, et al. Feeling of grief and loss in parental caregivers of adults diagnosed with intellectual disability. J Appl Res Intellect Disabil. 2021;34:712–23. https://doi.org/10.1111/jar.12842 .
O’Neill LP, Murray LE. Perceived parenting styles fail to mediate between anxiety and attachment styles in adult siblings of individuals with developmental disabilities. J Autism Dev Disorders. 2015;46:3144–54. https://doi.org/10.1007/s10803-016-2859-5 .
Schlebusch L, Dada S, Samuels AE. Family quality of life of South African families raising children with Autism Spectrum Disorder. J Autism Dev Disorders. 2017;47. https://doi.org/10.1007/s10803-017-3102-8 .,1966–1977.
Pillai S, Makhetha M, Aldous C. A study reflecting the demographics and comorbidities of children diagnosed with autism spectrum disorder at initial presentation to the KwaZulu-Natal Children’s hospital. S Afr J Child Health. 2021;15:3,125–9. https://doi.org/10.7196/SAJCH.2021.v15.i3.1752 .
Mulligan B, John M, Coombes R, Singh R. Developing outcome measures for a family intensive support service for children presenting with challenging behaviours. Br J Learn Disabil. 2014;43:161–7. https://doi.org/10.1111/bld.12091 .
Sajjad S. Stress faced by Pakistani mothers of children with intellectual disabilities and its impact on their family life. J Int Association Special Educ. 2011;12:171–78. http://iase.coe.nau.edu/index3.html .
Alaki SM, Bakry NS. Dental Pain in Children with Intellectual disabilities: caregivers’ perspective. Int J Dent. 2012. https://doi.org/10.1155/2012/701608 .
Frolova O, Nikolaev A, Grave P, Lyakso E. Speech Features of Children with Mild Intellectual Disabilities. In International Conference on Multimodal Interaction, 23,0 ,9–13; https://doi.org/10.1145/3610661.3616236 (2023).
Robinson T, Wakely L, Marquez J, Rae K. Surviving, not thriving: a qualitative analysis of parents’ perceptions of physical activity participation for rurally residing children with a disability. Rural Remote Health. 2018;18:4536. https://doi.org/10.22605/RRH4536 .
Clasquin-Johnson MG, Clasquin-Johnson M. How deep are your pockets? Autoethnographic reflections on the cost of raising a child with autism’. Afr J Disabil. 2018;7(0):a356. https://doi.org/10.4102/ajod.v7i0.356 .
McKenzie JA, Abrahams T, Adnams C, Kleintjies S. The intellectual disability in South Africa: the possibilities and limits of democratic rights. Tizard Learn Disabil Rev. 2019;24:4,204–12. https://doi.org/10.1108/TLDR-04-2019-0015 .
Download references
Acknowledgements
The authors would like to acknowledge O.N. Makhubela-Nkondo as a PhD supervisor of one of the authors.
The research received funding from the University of South Africa as PhD bursary.
Author information
Authors and affiliations.
School of Nursing, Faculty of Health Sciences, University of Free State, Nelson Mandela Drive, 9301, Bloemfontein, Free State Province, South Africa
Mantji Juliah Modula & Mpho Grace Chipu
You can also search for this author in PubMed Google Scholar
Contributions
Modula MJ conceptualized the study, developed the protocol and interview checklist, conducted the interviews, transcribed the data, analysed and drafted the manuscript and accept personal accountability to the findings of the study. Chipu MG reviewed and aligned a draft of the manuscript to the journal.
Corresponding author
Correspondence to Mantji Juliah Modula .
Ethics declarations
Ethics approval and consent to participate.
The study received ethical clearance approval to commence with the empirical data collection process from the Research Ethics Committee (REC) Department of Health Studies, University of South Africa (reference number, HSHDC/860/2018) (2018). The study further received formal written permissions to collect data at Capricorn District sites from the Limpopo Department of Health (reference number LP_2018_07_014) (2018) and Capricorn Health District (reference number S.5/3/1/2) (2018). The participants signed written informed consent to participate in the study. The researcher maintained the confidentiality and privacy of all participants throughout the study. The researcher ensured safe data storage, and no unauthorised persons could access it.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Modula, M.J., Chipu, M.G. Exploring information needs among family caregivers of children with intellectual disability in a rural area of South Africa: a qualitative study. BMC Public Health 24 , 1139 (2024). https://doi.org/10.1186/s12889-024-18606-7
Download citation
Received : 10 July 2023
Accepted : 09 April 2024
Published : 24 April 2024
DOI : https://doi.org/10.1186/s12889-024-18606-7
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Information needs
- South Africa
BMC Public Health
ISSN: 1471-2458
- Submission enquiries: [email protected]
- General enquiries: [email protected]
This paper is in the following e-collection/theme issue:
Published on 23.4.2024 in Vol 26 (2024)
This is a member publication of University of Oxford (Jisc)
Empowering School Staff to Support Pupil Mental Health Through a Brief, Interactive Web-Based Training Program: Mixed Methods Study
Authors of this article:
Original Paper
- Emma Soneson 1, 2 , PhD ;
- Emma Howarth 3 , PhD ;
- Alison Weir 4, 5 , MA, MSc ;
- Peter B Jones 2 * , PhD ;
- Mina Fazel 1 * , DM
1 Department of Psychiatry, University of Oxford, Oxford, United Kingdom
2 Department of Psychiatry, University of Cambridge, Cambridge, United Kingdom
3 School of Psychology, University of East London, London, United Kingdom
4 Faculty of Education, University of Cambridge, Cambridge, United Kingdom
5 Howard Community Academy, Anglian Learning multi-academy trust, Bury St Edmunds, United Kingdom
*these authors contributed equally
Corresponding Author:
Emma Soneson, PhD
Department of Psychiatry
University of Oxford
Warneford Lane
Oxford, OX3 7JX
United Kingdom
Phone: 44 1865 613127
Email: [email protected]
Background: Schools in the United Kingdom and elsewhere are expected to protect and promote pupil mental health. However, many school staff members do not feel confident in identifying and responding to pupil mental health difficulties and report wanting additional training in this area.
Objective: We aimed to explore the feasibility of Kognito’s At-Risk for Elementary School Educators , a brief, interactive web-based training program that uses a simulation-based approach to improve school staff’s knowledge and skills in supporting pupil mental health.
Methods: We conducted a mixed methods, nonrandomized feasibility study of At-Risk for Elementary School Educators in 6 UK primary schools. Our outcomes were (1) school staff’s self-efficacy and preparedness to identify and respond to pupil mental health difficulties, (2) school staff’s identification of mental health difficulties and increased risk of mental health difficulties, (3) mental health support for identified pupils (including conversations about concerns, documentation of concerns, in-class and in-school support, and referral and access to specialist mental health services), and (4) the acceptability and practicality of the training. We assessed these outcomes using a series of questionnaires completed at baseline (T1), 1 week after the training (T2), and 3 months after the training (T3), as well as semistructured qualitative interviews. Following guidance for feasibility studies, we assessed quantitative outcomes across time points by comparing medians and IQRs and analyzed qualitative data using reflexive thematic analysis.
Results: A total of 108 teachers and teaching assistants (TAs) completed T1 questionnaires, 89 (82.4%) completed T2 questionnaires, and 70 (64.8%) completed T3 questionnaires; 54 (50%) completed all 3. Eight school staff members, including teachers, TAs, mental health leads, and senior leaders, participated in the interviews. School staff reported greater confidence and preparedness in identifying and responding to mental health difficulties after completing the training. The proportion of pupils whom they identified as having mental health difficulties or increased risk declined slightly over time (median T1 =10%; median T2 =10%; median T3 =7.4%), but findings suggested a slight increase in accuracy compared with a validated screening measure (the Strengths and Difficulties Questionnaire). In-school mental health support outcomes for identified pupils improved after the training, with increases in formal documentation and communication of concerns as well as provision of in-class and in-school support. Referrals and access to external mental health services remained constant. The qualitative findings indicated that school staff perceived the training as useful, practical, and acceptable.
Conclusions: The findings suggest that brief, interactive web-based training programs such as At-Risk for Elementary School Educators are a feasible means to improve the identification of and response to mental health difficulties in UK primary schools. Such training may help address the high prevalence of mental health difficulties in this age group by helping facilitate access to care and support.
Introduction
In recent years, there has been an increased emphasis on the role of schools in supporting children’s mental health [ 1 - 3 ]. This enhanced focus has been driven in large part by an apparent increase in mental health difficulties (including behavioral, social, and emotional difficulties) present in school-aged populations [ 4 - 6 ]—a concern that became increasingly prominent in the context of the COVID-19 pandemic and the associated school closures and social distancing measures [ 7 , 8 ]. There is also a growing recognition of the many unique advantages of using the school setting to promote and protect pupil mental health [ 9 ]. First, most lifetime disorders begin during the schooling years [ 10 ], which suggests that schools may be an ideal setting for early identification and intervention. Second, schools have access to most children, meaning that they are an important component of any public health approach to address child mental health difficulties [ 11 - 14 ]. Third, schools benefit from prolonged engagement with pupils, which can facilitate the implementation of mental health promotion and prevention strategies as well as support and interventions for pupils with identified mental health needs [ 12 ]. Finally, mental health support in schools is often more accessible to families than other types of support [ 15 ].
However, while school staff are increasingly expected to support children’s mental health [ 1 ], many do not feel prepared to do so [ 16 - 19 ] due in part to receiving limited training and supervision in this area [ 20 ]. Therefore, improving school staff’s confidence and preparedness are important considerations for supporting them in taking an expanded role in pupil mental health [ 21 ]. Most schools offer some form of mental health training [ 22 , 23 ], but many staff members believe that they could benefit from additional training [ 18 - 20 , 24 - 26 ]. One area where staff training may be particularly beneficial is the identification of and first response to pupils who have mental health difficulties or who are believed to be at increased risk of developing them. However, although there is evidence suggesting that school staff, parents, and practitioners see such training as an acceptable, feasible, and potentially useful way to support pupil mental health [ 20 , 27 - 29 ], empirical evidence for the effectiveness of such training is limited and focuses primarily on intermediate outcomes (eg, staff knowledge and confidence) rather than downstream outcomes (eg, accurate identification, access to support, and mental health outcomes) [ 30 , 31 ]. Furthermore, there are several potential barriers to implementing training programs in schools, including time, cost, and resource requirements [ 28 ].
At-Risk for Elementary School Educators : A Brief, Interactive Web-Based Training
Training programs that address these barriers may be beneficial for supporting schools in identifying and responding to pupil mental health difficulties. Brief, interactive web-based training programs are a particularly promising avenue as they have the potential to be more affordable, flexible, and scalable than other training formats. One such training is At-Risk for Elementary School Educators (hereinafter, At-Risk ), a virtual simulation-based program developed by the American company Kognito [ 32 ]. The program, which has been completed by >125,000 teachers in the United States, aims to improve pupil mental health by “[building] awareness, knowledge, and skills about mental health, and [preparing] users to lead real-life conversations with pupils, parents, and caregivers about their concerns and available support” [ 33 ].
The program addresses many common implementation barriers to school-based mental health training. For example, At-Risk only requires approximately 1 hour to complete, which is much shorter than many other available training programs [ 31 , 34 ]. This comparatively low time commitment may address the concern that training programs are overly time intensive and, thus, make the training more feasible for busy schools [ 28 , 34 , 35 ]. The web-based format of At-Risk may also address concerns about school-based mental health programs being resource intensive [ 28 ]. Nearly all school mental health training programs documented in the literature are face-to-face sessions led by external facilitators [ 34 , 36 ], with only a few examples of web-based training [ 37 - 39 ]. For schools with limited budgets, programs requiring external facilitators can prove unsustainable and have limited scalability. In terms of financial resources, the costs of At-Risk vary depending on the number of licenses purchased, but the maximum cost is approximately £22 (US $30) per user, a price point that is feasible for many UK schools. In the United States, there have been many examples of bulk purchases at the district or state level that have made the training even more affordable per teacher. In many areas, the training is even free at point of use due to state- or district-wide licensing agreements [ 40 ].
To date, 3 randomized studies have examined the effectiveness and acceptability of At-Risk among samples of American teachers [ 17 , 41 ] and teachers in training [ 42 ] across school years. Each study found high satisfaction ratings, with between 75% and 85% of participants rating the training as useful, well constructed, relevant, and easy to use, and nearly all (88%-95%) reporting that they would recommend it to colleagues. The training also improved teachers’ self-rated preparedness, self-efficacy, and likelihood of identifying and discussing concerns about pupils’ mental health and referring them to appropriate support when needed. These improvements were reflected in the teachers’ behaviors—compared with teachers in the control group , those who completed At-Risk self-reported significantly more helping behaviors (eg, identifying psychological distress, discussing concerns with pupils and parents, and consulting with parents about options for care and support) and gatekeeping behaviors (ie, connecting pupils with care and support) after the training and at 3 months after the training. The findings of these studies indicate that At-Risk may help improve teachers’ ability to identify and respond to pupil mental health needs and lead to positive behavior change in terms of discussing concerns and facilitating access to care and support.
At-Risk in a UK Context: Considerations for Transportability
These 3 studies suggest that At-Risk may be a promising intervention for improving children’s mental health; however, there is still much to be learned about the training’s effectiveness, feasibility, and acceptability. Furthermore, to date, no evaluation of the training has been conducted outside the United States. There is increasing focus on the influence of context on the effectiveness of complex interventions [ 43 - 48 ], and while some interventions have shown success in terms of transportability [ 48 ], other interventions that have evidence of effectiveness in one context have demonstrated null or even negative effects in another [ 46 ]. Furthermore, information that could inform “transportability” is often not collected as part of evaluations [ 44 ], making it difficult to determine the likelihood of success in a new setting.
There are many contextual differences between the United States and the United Kingdom that could mean that school-based interventions developed in one country may not translate well to the other. Cross-country differences in education systems and (mental) health services are particularly relevant to this study. Differences in the education system include the length and content of initial teacher training, the number and roles of teaching assistants (TAs), and school funding structures. There are also key differences in the structure and availability of school-based mental health provision. In the United States, schools often have staff whose sole or at least main responsibility is mental health, such as school psychologists. While these roles are becoming more common in the United Kingdom with the implementation of the Green Paper recommendations [ 1 ], in most UK primary schools, mental health is included within the broader roles of the special educational needs coordinator (SENCo) and pastoral team. Finally, differences in the wider health care systems across the countries also mean that the process and outcomes of external referrals to specialist mental health services vary across settings, another fact that may influence the transportability of school-based interventions such as At-Risk.
Given these uncertainties regarding intervention transportability, additional evaluation of At-Risk is needed to understand whether it is a potentially useful and feasible tool to improve the identification of and response to mental health difficulties in UK primary schools. To explore the potential value of the training in this new context, we conducted a mixed methods feasibility study of At-Risk in 6 UK primary schools covering pupils aged 4 to 11 years . We aimed to examine the influence of At-Risk on staff confidence and preparedness, identification of pupils with mental health difficulties or increased risk of developing mental health difficulties, mental health support outcomes for identified children, and intervention acceptability and practicality.
Study Design
We used a mixed methods, nonrandomized, pretest-posttest study design to explore the feasibility of At-Risk in UK primary schools. While feasibility studies are acknowledged as a key stage of intervention design and evaluation [ 49 , 50 ], there is no universally agreed-upon definition of a feasibility study [ 50 , 51 ]. Therefore, we focused on 3 criteria from the guidance by Bowen et al [ 52 ]: acceptability, practicality, and limited effectiveness testing.
Intervention: At-Risk for Elementary School Educators
At-Risk is a web-based training that is delivered individually and requires only a log-in and internet connection. Using a simulation-based teaching model, the training aims to (1) improve mental health awareness and knowledge, (2) empower users to approach pupils about what they have noticed, (3) impart skills to have meaningful conversations with pupils and parents, and (4) train users to refer pupils to further support. The diagram in Figure 1 illustrates how the training might lead to improved mental health outcomes for pupils.
The simulation begins with an introduction by a virtual coach, who defines and explains how to recognize the warning signs of psychological distress and specific mental health difficulties and provides guidance and practical advice for discussing and acting upon concerns. Users then practice 2 virtual scenarios. The first scenario involves a fifth-grade (UK Year 6; ages of 10-11 years) teacher speaking with the parent of a pupil showing signs of behavioral difficulties. The second involves a third-grade (UK Year 4; ages of 8-9 years) teacher speaking with a pupil showing signs of emotional difficulties. During the conversations, users choose what to say via drop-down menus organized into categories (eg, “bring up concerns” or “ask a question”) and phrases (eg, “Mia sometimes seems a little agitated in class”). Throughout the conversation, users receive feedback through a “comfort bar” (based on how the pupil or parent perceives the conversation), opportunities to “see” the thoughts of the pupil or parent, and suggestions from the virtual coach.
Importantly, there is no one “right” way to conduct the conversations, and several approaches can lead to a positive outcome. Throughout the conversation, users can “undo” actions to backtrack after receiving an undesirable response or to explore what the response would have been had they chosen another option. At the end of each conversation, the pupil or parent provides feedback on the conversation. The training finishes with a short segment on connecting pupils with further support.
For this feasibility study, we used an unmodified version of the training (ie, the standard training designed for American schools, not tailored to the UK context) provided free of cost by Kognito. The potential need for adaptation and tailoring was an important consideration that we explicitly examined as part of our exploration of the acceptability and practicality of At-Risk in this new setting.

Recruitment
We originally sought to purposively sample 5 primary schools from Cambridgeshire or Norfolk that (1) had a higher-than-average proportion of pupils eligible for free school meals or (2) were located in an area in the top tertile of deprivation as measured using the Index of Multiple Deprivation [ 53 ], which we calculated with the publicly available Schools, pupils and their characteristics data [ 54 ]. We emailed headteachers, SENCos, and mental health leads from 131 candidate schools in September and October 2019 about participating in the study. To increase recruitment, we contacted additional schools in January 2020 for a study start date of March 2020. However, the study was suspended in March 2020 due to the in-person school closures associated with the onset of the COVID-19 pandemic. As some of the participating schools dropped out due to the pandemic, we reopened recruitment for a January 2021 study start date. In this round, we did not restrict participation by the 2 deprivation criteria described previously (ie, free school meal eligibility and Index of Multiple Deprivation), so any UK-based mainstream primary school was eligible to participate. The January 2021 start date was again delayed by the pandemic, but there was no subsequent recruitment.
Teachers and TAs
Schools were responsible for recruiting individual teachers and TAs to participate in the training. We encouraged schools to invite all teachers and TAs to participate, but schools made a variety of decisions in this regard. Three schools (schools D, E, and F) had all staff complete the training during inset (in-service training) days or other designated times, 2 schools (schools A and C) had staff volunteer to participate, and 1 school (school B) selected 2 to 3 staff members in each year group to participate.
Measures and Materials
School characteristics.
The characteristics of the participating schools, including school type, school sex (ie, whether they were single or mixed sex), urbanicity, head count, area-level deprivation, level of free school meal eligibility, ethnic composition, and proportion of pupils with special educational needs, were obtained from publicly available data from the Department for Education [ 54 , 55 ].
Teacher and TA Identification Form
The purpose of the Teacher and TA Identification Form ( Multimedia Appendix 1 ) was to understand which pupils participants would identify as having mental health difficulties or an increased risk of developing mental health difficulties. As systematic reviews in this area have identified no suitable questionnaires [ 28 , 30 ], we developed a bespoke questionnaire, which was reviewed by a school staff advisory group to ensure accuracy and relevance. The questionnaire begins with instructions, including explanations and examples of what is meant by “mental health difficulties or risk for mental health difficulties.” Full definitions are provided in Multimedia Appendix 1 , but in brief, “mental health difficulties” are described as “behavioural and social-emotional problems” regardless of formal diagnosis, and “risk for mental health difficulties” is described as experiences that increase the chance of a child developing mental health difficulties in the future.
For all pupils in their class, participants first indicated whether they thought a pupil had mental health difficulties or increased risk. If yes, they answered 9 subsequent questions about mental health support outcomes. The first four outcomes were about communication of concerns, namely whether they had (1) formally documented their concerns with the school, (2) communicated concerns to the SENCo, pastoral care lead, or mental health lead, (3) communicated concerns to another member of the school staff, or (4) communicated concerns to the child or their parents. The next five outcomes pertained to the provision of mental health support, namely whether the pupil (5) received in-class support; (6) received in-school support or had an in-house support plan; (7) had documented social, emotional, and mental health (SEMH) status (a type of special educational need focused on mental health difficulties); (8) had been referred to external mental health services; or (9) had access to external mental health services.
Strengths and Difficulties Questionnaire
The teacher-report Strengths and Difficulties Questionnaire (SDQ) [ 56 - 59 ] served as the comparator for findings about teachers’ and TAs’ identification of pupils. The SDQ includes 25 positive and negative psychological attributes across 5 scales: emotional symptoms, conduct problems, hyperactivity/inattention, peer relationship problems, and prosocial behavior. The first 4 scales add up to a Total Difficulties Score (0-40, with higher scores representing greater difficulties). The SDQ has demonstrated acceptable psychometric properties in primary school samples [ 60 ]. It is important to note that the SDQ is not an exact comparator as it measures a narrower concept than the Teacher and TA Identification Form (which also includes increased risk ). However, this comparison could potentially yield valuable information regarding feasibility .
Pre- and Posttraining Surveys
Kognito uses pre- and posttraining surveys to assess their training. These surveys (based on the validated Gatekeeper Behavior Scale [ 61 ]) explore teachers’ self-efficacy in identifying and responding to mental health difficulties and whether their attitudes, self-efficacy, or practice have changed since completing the At-Risk training. The posttraining survey also includes questions on perceptions of the training’s impact. We independently (ie, with no input from Kognito) reviewed the merits of these questionnaires and decided to use them in this study because (1) they covered relevant and useful concepts related to our aims and (2) using them increased comparability to the other 3 US-based studies of At-Risk . We slightly adapted the surveys to make them more relevant to the UK context ( Multimedia Appendix 2 ).
Interview Schedules
For the pretraining interviews with SENCos and mental health leads, we developed a topic guide about current practice ( Multimedia Appendix 3 ) with the specific purpose of creating Mental Health Resource Maps for each school (refer to the Procedures section). The main topics pertained to formal and informal procedures for when staff members suspect that a child might have mental health difficulties or increased risk, as well as the types of support available.
For the posttraining interviews with teachers, TAs, and strategic stakeholders (ie, those with key leadership roles, including senior leadership teams [SLTs], school governors, and SENCos and mental health leads), we developed 3 separate topic guides ( Multimedia Appendix 3 ), which were informed by our research questions, systematic reviews [ 28 , 30 ], and the Consolidated Framework for Implementation Research [ 62 , 63 ]. For teachers and TAs who completed At-Risk and strategic stakeholders, interview topics included the acceptability of the training, the practicality of implementing it in schools, the utility of further refinement and testing, possible harms associated with the training (if any), and suggestions for adaptations. For teachers and TAs who did not complete the training, topics included reasons for not completing it, barriers to acceptability and practicality, and suggestions for adaptations.
Interviews With SENCos and Mental Health Leads
We conducted a pretraining interview with each school’s SENCo or mental health lead to develop a “Mental Health Resource Map” with information on referral processes and available support. These maps served an ethical purpose by ensuring that pupils identified as potentially having mental health difficulties would have the best possible chance of being linked to care and support.
Completing At-Risk
Schools’ timelines for the study varied due to the pandemic and other commitments. School D completed the training in December 2020; school E completed the training in March 2021; schools B, C, and F completed the training in May 2021; and school A completed the training in June 2021. At baseline (T1), participants completed a Teacher and TA Identification Form and the pretraining survey. They then completed the At-Risk training. We encouraged schools to designate specific time for the training, which 3 schools (schools D, E, and F) did. One week after training (T2), participants were asked to complete a second Teacher and TA Identification Form and the posttraining survey. Three months after the training or at the end of the school year (whichever came first; T3), participants completed a third Teacher and TA Identification Form as well as SDQs for all pupils. All questionnaires were completed on the University of Cambridge Qualtrics platform (Qualtrics International Inc).
Feedback Provision
After T2, we provided all SENCos and mental health leads but not teachers or TAs with feedback regarding which children had been identified as having mental health difficulties or increased risk. After T3, we provided SDQ scores for each child as well as whole-class distributions (where available). This feedback was provided to ensure the ethical conduct of the study.
Interviews With Teachers, TAs, and Strategic Stakeholders
We aimed to recruit at least 3 teachers or TAs who completed the training per school, 3 to 5 teachers or TAs who had not completed the training across all schools, and up to 3 strategic stakeholders per school for posttraining semistructured interviews. Schools contacted staff members directly with an invitation to complete a virtual interview.
Quantitative Outcomes
Analytical samples.
For the main analysis, participants were included if they (1) completed at least the pretraining (T1) questionnaires and the training itself and (2) had what we judged to be a typical number of children they regularly worked with. For the latter criterion, given that the average UK primary school class size is approximately 27 to 28 pupils [ 64 ], we excluded teachers and TAs who worked with <10 children (as we suspected this would not be a random selection of pupils and would therefore influence aggregate identification rates) and those who worked with >60 children (as we believed that it would be difficult for a teacher or TA to know >2 classes’ worth of children well enough to make accurate judgments about their mental health).
Teacher and TA Self-Efficacy and Preparedness
To assess teachers’ and TAs’ preparedness, self-efficacy, and perceptions of training impact, we calculated the absolute and relative frequencies of responses to the pre- and posttraining surveys. Participants were eligible for inclusion in this analysis only if they had pretraining (T1) data.
Identification Outcomes
On the basis of the Teacher and TA Identification Forms, we calculated the number and percentage of pupils in each class whom teachers and TAs perceived as having mental health difficulties or increased risk at each time point. We summarized these across all participants using medians and IQRs.
We then calculated SDQ scores, which we compared with responses from the Teacher and TA Identification Form by calculating (1) the median and IQR for the percentage of children identified by participants who did not have elevated SDQ scores and (2) the median and IQR for the percentage of children with elevated SDQ scores who were not identified by participants. To be included in these analyses, participants had to have completed all 3 time points. For the first outcome, they had to have completed an SDQ for all children they identified in the Teacher and TA Identification Form . For the second outcome, they had to have completed SDQs for at least 80% of their class. Where it was possible to match pupil IDs between teachers and TAs, we pooled SDQ data such that, if one participant did not meet the inclusion criteria themselves, they could still be included if the SDQ data were available from another staff member working with the same children.
Mental Health Support Outcomes
Finally, for each time point, we calculated medians and IQRs for the proportion of identified children with each of the 9 mental health support outcomes (refer to the Teacher and TA Identification Form section for the outcomes) .
Sensitivity Analyses
We also conducted 2 post hoc sensitivity analyses. The first sensitivity analysis excluded all participants from school D. When we prepared feedback for school D (the first school to complete the training), we learned that most participants at the school had misinterpreted the Teacher and TA Identification Form. We edited the form and instructions accordingly to address this issue, but therefore, school D participants completed a slightly different form than the other schools. The second sensitivity analysis was a complete case analysis intended to explore observed differences in outcomes according to whether participants had completed all 3 time points. For the analysis of outcomes pertaining to preparedness, self-efficacy, and perceptions of training impact, we included all participants who completed the surveys at least at T1 and T2.
Statistical Analysis
For all quantitative outcomes, we focused on preliminary, descriptive comparisons across the 3 time points and did not perform any formal hypothesis testing. This aligns with established recommendations for feasibility studies, which generally lack the statistical power necessary for a clear interpretation of hypothesis-testing results [ 65 - 68 ]. We conducted all quantitative analyses in R (version 4.0.3; R Foundation for Statistical Computing) [ 69 ] except for the comparison of Teacher and TA Identification Forms and SDQ scores, for which we used Microsoft Excel (Microsoft Corp). We created all plots using the ggplot2 [ 70 ] and likert packages [ 71 ]. To score the SDQs, we used the freely available R code on the Youthinmind website [ 72 ].
Qualitative Outcomes
We considered 3 analysis approaches for the interview and qualitative questionnaire data: content analysis [ 73 ], framework analysis [ 74 ], and reflexive thematic analysis [ 75 , 76 ]. We initially decided to use content analysis for the survey comments and reflexive thematic analysis for the interviews; however, as we familiarized ourselves with the data, we realized that there was significant overlap between the survey comments and interviews and decided that analyzing them separately was not a useful distinction. As our main aim was to generate insights into the program and its future potential, we decided to use the 6-phase reflexive thematic analysis by Braun and Clarke [ 76 ] for all qualitative data due to its flexibility and ability to generate themes both inductively and deductively. ES developed the initial themes, and MF and EH helped clarify and enrich them. ES and MF worked together to name and refine the themes before the final write-up. We managed and coded all qualitative data in ATLAS.ti (version 9.1.3; ATLAS.ti Scientific Software Development GmbH) and additionally created manual thematic maps to better visualize and understand patterns between our data.
Ethical Considerations
This study was approved by the University of Cambridge Psychology Research Ethics Committee (PRE 2019.076). We obtained active informed consent from all teachers and TAs who took part in the study. We used an opt-out model for parental consent whereby parents received (directly from the schools via their preferred communication routes) an information sheet detailing study aims, procedures, how data would be used, and the right to opt their child out of participation. Parents had 2 weeks to opt their child out of the study by returning a hard copy of the opt-out form or emailing or calling the school. Schools kept track of all opt-outs and instructed teachers and TAs not to include these children in their forms. All quantitative data were collected using anonymous pupil and staff identifiers generated by the participating schools, and all qualitative data were deidentified before analysis, with identifiable information stored on secure servers at the University of Cambridge. Teachers and TAs received £20 (approximately US $28) vouchers for completing the training and questionnaires for at least 2 of the 3 time points and an additional £10 (approximately US $14) for taking part in an interview. School staff members who created the anonymous identifiers received £10 (approximately US $14) vouchers to thank them for their time.
Participants
A total of 6 schools participated in this study (Table S1 in Multimedia Appendix 4 [ 40 ]). Among these 6 schools, there were 4 (67%) from Cambridgeshire and 1 (17%) each from Greater London and Merseyside; 5 (83%) were located in urban areas and 1 (17%) was located in a rural area. All but 1 school (5/6, 83%) were situated in areas of above-average deprivation, and 50% (3/6) of the schools had a higher-than-average proportion of pupils eligible for free school meals. In total, 67% (4/6) of the schools had a high proportion of White pupils (>80%), and 33% (2/6) of the schools were more diverse, with approximately 20% of pupils from Black, Black British, Caribbean, or African backgrounds (school B) or Asian or Asian British backgrounds (school E).
A total of 108 teachers and TAs completed the T1 questionnaires and the training itself, 89 (82.4%) completed the T2 questionnaires, and 70 (64.8%) completed the T3 questionnaires ( Table 1 ), with 54 (50%) having completed all 3. After excluding those teachers and TAs who did not meet the inclusion criteria for the analyses, the final analytical samples were as follows:
- Main analysis of identification and mental health support outcomes: n=97 at T1, n=75 at T2, and n=57 at T3.
- Main analysis of preparedness, self-efficacy, and training impact outcomes: n=107 at T1 and n=83 at T2.
- Main analysis comparing identification outcomes with SDQ scores: n=28 and n=25 (refer to the following section).
- Complete case sensitivity analysis: n=51 at T1, T2, and T3.
- Sensitivity analysis excluding all teachers and TAs from school D: n=70 at T1, n=54 at T2, and n=41 at T3.
Compared with the 2019-2020 national workforce statistics for teachers and TAs working in state-funded nursery and primary schools [ 77 ], our sample had a similar proportion of women (81/89, 91% in our sample vs 90.9% nationally) and a slightly higher proportion of White staff members (82/89, 92% in our sample vs 90.5% nationally).
A total of 7.4% (8/108) of school staff members from 67% (4/6) of the schools completed an interview ( Table 2 ).
a N=89 because this information was collected only at T2.
b N NA =4 (number with missing data for this question).
c Percentages add up to >100 because some participants had multiple roles.
d SENCo: special educational needs coordinator.
e N NA =7 (number with missing data for this question).
a PSHE: Personal, Social, Health and Economic.
b SENCo: special educational needs coordinator.
c TA: teaching assistant.
d HLTA: higher-level teaching assistant.
Pretest-posttest changes suggested that participating in the training was beneficial for the staff and that they had positive perceptions of the training. Findings regarding preparedness ( Figure 2 ) suggest improvements across all domains of recognizing and acting upon concerns about pupils’ mental health, particularly in terms of using key communication strategies and working with parents. Findings regarding self-efficacy ( Figure 3 ) suggest that participants were more confident in their abilities to discuss their concerns about pupils’ mental health after the training than before. Again, the largest changes were observed in discussing concerns with parents and applying key communication strategies. Finally, findings regarding teachers’ and TAs’ perceptions of the impact of applying the skills of the training ( Figure 4 ) suggest that they were generally positive about the possible effects of the training on pupil outcomes (ie, attendance and academic success), teacher-pupil rapport, and the classroom environment. The results from the complete case analysis ( Multimedia Appendix 5 ) were nearly identical to those of the main analysis (all differences were ≤3 percentage points in magnitude).

In terms of how many pupils were identified as having mental health difficulties or increased risk, participants identified similar proportions of their pupils before and immediately after the training and then fewer over time. The median percentage of pupils whom participants believed had mental health difficulties or increased risk was 10% (IQR 6.7%-18.2%) at T1, 10% (IQR 4.5%-16.7%) at T2, and 7.4% (IQR 5.0%-16.7%) at T3. The directions of change were similar for both sensitivity analyses (whereby teachers and TAs identified fewer children over time), with slight differences. For the sensitivity analysis excluding school D ( Multimedia Appendix 6 ), the percentages were slightly (approximately 2 percentage points) higher. For the complete case analysis, the decrease was also notable 1 week after the training, decreasing from 10% (IQR 6.7%-17.3%) at T1 to 8% (IQR 3.9%-16.7%) at T2 and 7.4% (IQR 5.7%-16.7%) at T3.
In terms of the accuracy of identification, it seems that teachers and TAs became slightly more accurate over time in comparison to pupils’ SDQ scores (although it is important to acknowledge the limitations described in the Methods section regarding questionnaire comparability). The median percentage of children identified by participants who did not have elevated SDQ scores was 40% (IQR 0%-50%) at T1, 27.2% (IQR 0%-50%) at T2, and 25% (IQR 0%-50%) at T3. The median percentage of children with elevated SDQ scores who were not identified by participants was 68.8% (IQR 42.9%-87.5%) at T1, 66.7% (IQR 50%-88.2%) at T2, and 57.1% (IQR 33.3%-87.5%) at T3. In the sensitivity analysis excluding school D, the results were similar (typically within 5 percentage points); one small difference was that the median percentage of children identified by teachers and TAs who did not have elevated SDQ scores was 0% (IQR 0%-50%) at T2. The results of the complete case analysis were identical to those of the main analysis.
Overall, the findings suggest that the training may be beneficial for facilitating conversations and access to school-based support (but not external support) for pupils with identified mental health difficulties or increased risk. Figure 5 presents the findings for the 9 mental health support outcomes among identified children across the 3 study time points. As with before the training, there was typically a wide variation in outcomes.
A comparison across time points suggests that participants formally documented their concerns and spoke with the SENCo, pastoral lead, or mental health lead for a greater proportion of identified pupils after the training than before. For example, at T1, teachers and TAs documented concerns for a median of 50% (IQR 0%-100%) of identified pupils; this increased to 56.3% (IQR 4.2%-100%) at T2 and 75.7% (IQR 0%-100%) at T3. The equivalent statistics for speaking with the SENCo, pastoral lead, or mental health lead were a median of 66.7% (IQR 16.7%-100%) at T1, 75% (IQR 50.0%-100%) at T2, and 95.5% (IQR 50.0%-100%) at T3. There was no change in speaking with another staff member, but this was because nearly all participants did so across all time points. Finally, the percentage of pupils whom teachers and TAs spoke with (or whose parents they spoke with) also increased after the training, with a median of 33.3% (IQR 0%-87.5%) at T1, 61.9% (IQR 0%-100%) at T2, and 50% (IQR 0%-100%) at T3.
A comparison across time points also suggests increases in school-based support for identified children after the training compared with before. The median percentage of pupils identified by teachers and TAs who received in-class support increased from 75% (IQR 35.4%-100%) at T1 to 100% at T2 and T3 (IQR 50%-100% and 66.7%-100%, respectively). There was a more modest increase in the receipt of in-school support or in-house support plans, with a median of 40% (IQR 0%-71.4%) of identified pupils receiving them at T1 compared with 50% at T2 and T3 (IQR 3.6%-100% and 8.3%-81.4%, respectively). There was very little change in documented SEMH status or referral or access to specialist mental health services. For each of these outcomes, the median percentage of identified pupils was 0% across time points.
The findings from the sensitivity analyses were similar to those of the main analysis in terms of direction, although improvements across time in the complete case analysis ( Multimedia Appendix 5 ) tended to be more modest than for the main analysis.

Acceptability and Practicality
Quantitative findings.
Quantitative data from the posttraining survey showed that participants were generally positive about the training. Of the 83 participants who completed the survey, 53 (64%) rated it as “good” and 13 (16%) rated it as “very good.” An additional 17% (14/83) rated it as “fair,” 2% (2/83) rated it as “poor”, and 1% (1/83) as “very poor.” A total of 84% (70/83) of the teachers and TAs said that the scenarios in the training were relevant to them. Finally, most participants (74/83, 89%) would recommend the training to other educators.
Qualitative Findings
Qualitative data also suggested that school staff generally found the training practical and acceptable. We generated three themes from our survey and interview data:
- Individual fit: positive perceptions, self-efficacy, and change.
- Institutional fit: alignment with school values and context.
- Taking it forward: improvements and implementation.
Additional findings on possible harms are presented in Multimedia Appendix 7 .
Individual Fit: Positive Perceptions, Self-Efficacy, and Change
In general, participants perceived the program to be a “good fit” with their personal philosophies and practice. Regarding the training itself, many appreciated the included scenarios, particularly in terms of their relevance to their practice. The format of the training—primarily that it was web-based and required active role-play—was also viewed as useful, engaging, and novel and might have contributed to its perceived usefulness. For example, one teacher commented:
The interactive elements of the training were brilliant and something which I have never encountered before! [Survey respondent (SR) 56; school E]
One teacher and well-being lead described:
I think it definitely made you think. [...] you had to really think about what was being said and the response that you would give, reflecting back on sort of the knowledge that they’d given you beforehand, so I thought that was good. [Interviewee 1]
Other participants suggested that opportunities to practice skills during the training improved the likelihood of using those skills in day-to-day practice.
Participants also believed that they had learned a lot from the training, especially in terms of skills and strategies. These included but were not limited to the skills within the At-Risk “EASING” strategy (check your Emotions, Ask for permission, be Specific, use I statements, keep it Neutral, and show Genuine curiosity). Importantly, there was evidence that participants had also applied new skills. Several participants described having new conversations with pupils or parents facilitated by the skills and strategies from the training. For example, one teacher described:
It was that permission thing [...] I wanted to ask [a child] about his home life [...] and kind of he just cried and didn’t want to speak about it anymore, and then when I asked him if we were OK to talk about it, he said, “Actually no, because I think I’m going to cry again,” so then we left it. And then he came to me the following week, and [...] said, “Can we talk about it now?” [...] so actually me asking that, it was the wrong time for him to talk about it, he wasn’t ready, he would have just been emotional, and wouldn’t have been able to get his words out, and actually the week after, him coming to me and saying, “Can we have a little chat,” works perfectly [...] And now we’re more aware of his situation. [Interviewee 2]
This skill seems to have enabled this pupil to have this conversation with the teacher in a manner (in terms of time, place, and identified person) that suited him. Other participants provided similar examples, referencing how skills from the training had facilitated better outcomes.
However, it is important to note that the perceived usefulness of the training varied. Most notably, some participants indicated that their previous training or role made the training less impactful. Illustratively, when asked how the training had impacted their practice, one TA responded:
Having previously received similar training, due to my role, I do not have any recent cases where the training would have changed the way I carried out discussions. [SR 60; school E]
Institutional Fit: Alignment With School Values and Context
Sustainable school-based programs should also align with the values of the school more broadly. Participants often referenced the importance of schools’ prioritization of pupil mental health. For example, one teacher described:
[Mental health is] a conversation which is constantly ongoing and trying to constantly better our practices and make sure we’re looking after them as best as we can and spotting things as best we can as well. [Interviewee 3]
This description demonstrates how prioritizing mental health can promote the critical evaluation of related school practices as well as the additional provision of training opportunities. In many cases, support from the SLT led to formal recognition of pupil mental health within school policies or plans. One strategic stakeholder explained:
I think because our school have well-being and mental health as such a focus, SLT are very supportive of doing things like this and they’re very accommodating. So when I said we had the training and people were going to have to take part in the training, it was very flexible, although they had other ones lined up, they were quite happy to move things around to make things work. And I think, the fact it is such a priority in our school definitely makes that easier. [Interviewee 1]
In this school, mental health and well-being were one of three main school priorities. As indicated previously, direction setting from the SLT is key to ensuring momentum and impetus. However, as others noted, it is important that support from the SLT is genuine rather than being “just another tick box” (Interviewee 4) exercise.
Another facet of institutional fit pertained to the practical aspects of the training. Schools are time- and resource-limited settings, so mental health training needs to fit within this context. The format of At-Risk, especially its flexibility and relatively low time requirements, was viewed as beneficial, with comments such as “For the amount of time [...] I got a huge amount from it” (Interviewee 4). Others made direct comparisons with other training courses. For example, one higher-level TA had previously completed a 1-day, in-person training course with a similar purpose to that of At-Risk. While she preferred the in-person training, she listed the benefits of both types:
[In the in-person training] you can then query and question to your trainer, so you’ve got that interaction, so that obviously isn’t there, is it, on the computer one. [...] if I was looking from a management point of view, I would say, budgetary, I’m sure it’s cheaper [...] to use [At-Risk], not just cheaper as in [...] money, [...] but also cheaper in time [...] So probably if I was looking [...] with my management hat on, I would say the computer-based [training] would get the same message, or similar message, across for a wider audience for probably a cheaper cost. [Interviewee 7]
In terms of efficiency, this participant highlighted the favorable input-to-output ratio of At-Risk , which could allow more staff members to participate in training. This quote also highlights that schools could use At-Risk flexibly. For example, schools might assign staff members to different training programs based on their roles and previous experience, with more intensive, in-person training for staff members with more significant mental health roles and At-Risk for those with fewer responsibilities or less experience.
Taking It Forward: Improvements and Implementation
Participants offered key insights into how to take the training forward in terms of both changes to the training itself and how best to implement it, primarily by tailoring it to the UK context. In terms of language, there was some reference to the American accent, but more so, participants highlighted the need to adapt some of the terminology and signposting resources to reflect UK support systems. They also made suggestions about additional training that could be useful with different topics (such as bullying) and age groups (particularly for younger children).
In addition to improvements and adaptations to the training itself, participants illustrated the importance of implementation. A common theme was that, to maximize impact, the training should include follow-up discussions or live workshopping. One teacher suggested:
I think some kind of “live” element to conclude the training—to have a “real” person to ask questions to as part of a group video chat could have been useful. Also, maybe to ask advice about particular scenarios that we may have found ourselves in in the past. [SR 56; school E]
By facilitating greater engagement and critical thinking, a live element could enhance the impact of the training and potentially make At-Risk more acceptable to those who generally prefer face-to-face training. Participants indicated that someone internal, for example, the SENCo, would be best placed to lead a live element and would enable staff to practice role-playing based on situations and scenarios specific to each school.
There was also wide acknowledgment that any training had to lie within a strong support system. This began with having a clear referral pathway for identified concerns, which was viewed as important for facilitating access to support. In some cases, teachers and TAs were able to find new ways to support children after completing the training. However, in many cases, participants—and strategic stakeholders in particular—explained that support had not always been readily available. For example, one strategic stakeholder recounted what happened after the training:
A lot of them are people saying to me, “What are you going to do about it?” about different children. And I, because some of our support staff don’t know the sort of route for getting extra support, or they’re really shocked to find actually there’s nothing out there for these children...it’s about what we can do in school, and I think people have been really quite shocked about that. You know, they just presume I can make a phone call and these children will get face-to-face counselling. [Interviewee 5]
This shows the importance of embedding the training within a wider support system, including collaboration with external agencies. However, many interviewees referenced the systemic issues that schools face in helping pupils access specialist support, particularly in terms of the high thresholds and long waiting lists that exist for many external services. While schools may be able to provide beneficial support for children, particularly for those with lower-level difficulties, this indicates an ongoing area of need for schools and their pupils.
Summary of Findings
This study offers the first UK evidence for Kognito’s At-Risk for Elementary School Educators , extending findings from 3 US-based trials and providing needed evidence regarding the potential utility, acceptability, and practicality of brief, interactive web-based mental health training for school staff. Overall, the findings showed that At-Risk is a feasible means of improving the identification of and response to pupil mental health difficulties in UK primary schools. Quantitative findings showed that staff preparedness and self-efficacy in identifying and responding to mental health difficulties increased after the training. Identification rates did not increase (and, in fact, decreased at the 3-month follow-up), but there was some suggestion that teachers’ and TAs’ identification became slightly more accurate in comparison with SDQ scores. Crucially, for those pupils identified as having mental health difficulties or increased risk, in-school mental health support outcomes (ie, documentation or discussion of concerns, conversations with pupils and parents, and in-class and in-school support) increased after the training, but more “downstream” outcomes (ie, documented SEMH status and referral and access to external mental health services) did not. Qualitative findings indicated that participants generally found the training acceptable and practical, with many explaining how they intended to use or had already used the skills they learned to improve their practice. Participants also suggested several useful improvements for the training and its implementation, including making it more relevant to the United Kingdom, adding more scenarios, and including a live element in the implementation of the training.
Findings regarding confidence and preparedness reflect those of the 3 US-based studies of At-Risk [ 17 , 41 , 42 ] and the wider literature surrounding teacher mental health training [ 31 ]. In general, mental health training seems to be effective in improving staff confidence. For example, 2 Australian-based studies [ 37 , 78 ] found that secondary school teachers who completed training felt more confident discussing their concerns and helping pupils with their mental health. Another UK-based study of a psychoeducational training program to improve recognition of depression in secondary schools [ 79 ] found significant pretest-posttest improvements in teacher confidence in their knowledge of symptoms, ability to recognize symptoms, and knowledge about how to speak with pupils about their mental health. However, not all studies have shown an impact, with a prominent UK-based study of mental health first aid training finding no effect on educators’ confidence in helping pupils with their mental health [ 80 ].
The general decrease in the proportion of pupils identified as having mental health difficulties or increased risk stands in contrast to previous studies of At-Risk , which found that school staff identified significantly more pupils of concern after completing the training [ 17 , 41 ]. Evidence of the effect of other training programs on identification is extremely limited [ 30 , 31 , 36 ], and differences in context, training content and delivery, baseline knowledge, and outcome measurement make it difficult to compare findings across studies. Two vignette-based studies showed little effect of either mental health first aid [ 78 ] or psychoeducational [ 81 ] training on identification (although each study also reported high recognition of difficulties before the training), whereas studies focused on real-world identification have shown mixed results [ 79 , 82 ]. However, changes in the proportion of identified pupils must be contextualized within the accuracy of identification. There are consequences of both over- and underidentification [ 83 , 84 ], most notably in terms of inefficient allocation of limited mental health support resources. While comparison with the SDQ suggested that there was some improvement in terms of the accuracy of identification following the training, underidentification remained a substantial challenge, with between one-half and two-thirds of pupils with elevated SDQ scores remaining unidentified by teachers and TAs. The underidentification of children with mental health difficulties in educational settings, particularly for children with internalizing as opposed to externalizing problems [ 85 ], has been well documented in the literature [ 30 ], and it is likely that a combination of identification models is required to address this challenge [ 27 , 29 ].
Promisingly, the training appeared to be useful in terms of connecting pupils with care and support, an outcome not frequently measured in other studies [ 30 , 31 , 34 ]. First, the findings suggested that participants had conversations about or documented concerns for a greater proportion of identified pupils following the training, which reflects findings from previous studies of At-Risk [ 17 , 41 ]. This is a rather unique outcome in the literature as other training evaluations have found no difference between training and control groups in terms of conversations with pupils and colleagues [ 78 ]. Importantly, this study went beyond conversations to include outcomes pertaining to in-school and external support. The increases in in-class and in-school support for identified pupils reflect findings of the UK-based study by Kidger et al [ 80 ] of mental health first aid training and the Australian-based pilot study by Parker et al [ 37 ] of a web-based training program, each of which found a positive effect of the training on helping behaviors. Although in-class and in-school support seemed to increase following the training, it is notable that referrals and access to specialist services did not. There are several plausible explanations for this finding. For example, it is likely that school staff were already aware of children with the most severe mental health difficulties and were confident and able to support newly identified pupils—who might have had lower-level mental health difficulties—within the school setting. However, if the training did lead to the identification of children who might benefit from specialist care, there are many barriers to accessing such support (eg, availability and long waiting lists) that might have influenced these outcomes, as reflected in both the qualitative interviews and the wider literature [ 23 , 86 ].
In addition, quantitative and qualitative findings suggested that the program was a good fit for individuals and schools, which aligns with previous research on the acceptability and perceived need for mental health training for school staff [ 18 , 20 , 27 - 29 , 87 , 88 ]. The training’s format seemed to be a key contributor to its feasibility. With a few exceptions [ 37 , 39 , 89 ], the web-based simulation-based format of At-Risk is unique among training programs and is well aligned with teachers’ preferences. For example, in their focus group study of UK secondary school teachers, Shelemy et al [ 20 ] found that participants wanted engaging, interactive, and concise training that included practical strategies and illustrative case studies, all of which are central to At-Risk . While the authors found that teachers disagreed over the usefulness of web-based training, it is possible that these concerns would have decreased during the COVID-19 pandemic as staff became more accepting of web-based opportunities to learn.
Qualitative findings also demonstrated the importance of school context and culture, which have been highlighted in previous research [ 27 ]. In particular, participants noted the importance of school culture in adopting mental health interventions into regular practice. In their systematic review, Moore et al [ 90 ] identified school culture, values, and policies as key facilitators of sustaining mental health interventions. A related area of focus was support from the SLT. This support is a well-recognized factor contributing to intervention success and sustainability for several reasons, including these leaders’ practical role in communicating about interventions and allocating specific time and resources to them [ 43 , 90 , 91 ]. However, it is important to recognize that mental health training for school staff may be even more needed and impactful in schools where mental health is not as much of a priority.
Limitations
Our mixed methods approach, wide range of outcomes, and diverse sample of participating schools offer rich information regarding the feasibility of At-Risk in the United Kingdom. These strengths notwithstanding, there are also several limitations to consider when interpreting the findings. The nonrandomized design, while common for feasibility studies, prevents any conclusions regarding causality and also limits the exploration of other factors that may have influenced outcomes (eg, providing teachers and TAs with the Mental Health Resource Maps or SENCos and mental health leads with feedback on identified pupils). In terms of recruitment and retention, the study had 50% (54/108) attrition. Several factors may have influenced this, including the increased pressure on school staff due to the COVID-19 pandemic, the timing of the study within the school year, and the requirement to communicate with participants only via the study link person. While we tried to explore the effect of attrition through a complete case sensitivity analysis, we lacked important information on the characteristics of those who dropped out as this information was collected only at T2. Furthermore, we were only able to recruit 8 staff members for the posttraining interviews, which was far below our recruitment target. Low participation rates could again be due to several factors, including the impact of the COVID-19 pandemic or competing priorities. Of note, we were not able to recruit anyone who did not complete the training, any headteachers, or any staff from 2 of the schools (schools A and D). This could mean that we lack viewpoints that may be important for understanding the feasibility and utility of the training.
There were also limitations associated with the study measures. While the Teacher and TA Identification Form was informed by the literature and reviewed by our primary school staff advisory group, its validity and reliability are unknown. In addition, the questionnaire only measured mental health support outcomes for those pupils identified as having mental health difficulties or increased risk. Therefore, we do not have information on those who were not identified. The measure is also based on teacher and TA reports and so may not have complete information about all types of support that pupils receive. Another important limitation pertains to the comparator used to assess the identification outcomes. To understand the potential utility of the training program, it is important to have a robust comparator. While we chose to use the teacher-report SDQ, it would also have been interesting to compare identification outcomes with parent-rated mental health difficulties, particularly in light of the low interrater agreement of common measures of child mental health difficulties [ 92 ]. An even stronger comparator would be to assess the teacher and TA identification outcomes against a clinical interview; however, this was not feasible in this study.
Finally, at the time of writing, At-Risk is currently not available for use as Kognito restructures its offerings. This demonstrates a trend that unfortunately is a common occurrence in the field of mental health, whereby many evidence-based digital tools are not available to potential end users [ 93 ]. Nonetheless, the learnings from this feasibility study offer rich information on what type of content and format may be useful for training programs in this area and, as such, can support further development and evaluation in the field.
Implications for Practice
Studies have consistently demonstrated that school staff would appreciate additional training on how best to support pupil mental health [ 18 , 20 , 87 , 88 ]. However, to be scalable, such programs must be realistic in terms of time, cost, and resource requirements [ 28 , 90 , 91 ]. Contextualized within the wider literature on school-based mental health interventions, the findings from this study suggest that mental health training is a feasible option for upskilling school staff to identify and respond to pupil mental health difficulties. They further highlight several specific factors that might positively contribute to feasibility and scalability, many of which are reflected in the broader literature on mental health training [ 20 , 28 ]. For example, teachers and TAs appreciated that the training actively engaged them in learning and applying new skills and that it used realistic examples to demonstrate the real-world applicability of the training, whereas school leaders identified the relatively low time and cost requirements and flexibility as key factors that could make the training feasible for their school context.
However, this is not to say that there are no implementation barriers associated with At-Risk or similar training programs. While the resources required to implement At-Risk are relatively low compared with other training programs, they must still be considered within the context of other school priorities. As demonstrated in the interviews and the wider literature [ 3 , 43 , 90 , 91 ], support from school leadership is essential for securing the time and budget required to implement a training such as At-Risk , and in schools where mental health is not a priority, there are likely to be many barriers to implementation . Even in schools with strong support from the leadership team, it may be difficult to find the requisite budget, time, and human resources to devote to the training. Finally, as is the case with any school-based mental health intervention, it is important that schools do not take sole responsibility for pupils’ mental health. Active partnership between schools and mental health services is key to ensuring that schools feel empowered and supported in this role [ 21 , 90 , 94 ]. While the schools in this study worked hard to support pupils as best they could, interviewees expressed frustration about the difficulty of accessing external support for children who could benefit from it. This is not an uncommon theme in the wider literature surrounding school-based interventions [ 20 , 23 , 91 ] and is a key consideration for scaling up training programs.
Implications for Future Research
The promising findings of this study suggest that additional research is needed to explore the role of scalable mental health training in supporting schools to protect and promote children’s mental health. On the basis of gaps in the literature, particular areas of interest include training for primary school staff (as most are focused on secondary school staff), web-based training (as opposed to traditional time- and resource-intensive in-person training), and training that takes a “whole school approach” by including all school staff members (rather than only teachers). This final area is especially interesting as findings from this study and others [ 27 ] have highlighted stakeholders’ preference that training programs include all school staff members. While our study jointly analyzed findings for teachers and TAs, future research would do well to consider how the unique roles and perspectives of these professionals—as well as other staff members within the school setting—might influence outcomes. Furthermore, future research should be more inclusive about their choice of outcomes, as too often evaluations of school staff training programs have focused on intermediate outcomes such as knowledge or confidence [ 31 ] without considering more “downstream” outcomes such as access to support. Finally, as demonstrated in our study, there is great value in using mixed methods approaches and including information about wider issues of feasibility and implementation, and studies that take this broader lens can help identify programs that are scalable, sustainable, and effective.
Conclusions
School staff would welcome additional mental health training to enable them to respond to pupil mental health difficulties, but there are many barriers to implementing such training at scale. Therefore, training programs that have relatively low time and resource requirements have great potential to fulfill an unmet need in schools. This mixed methods feasibility study showed that At-Risk for Elementary School Educators —an example of a brief, interactive web-based training program—is a feasible means of empowering school staff to accurately identify and respond to pupil mental health difficulties and increased risk.
Acknowledgments
The authors would like to thank Professor Paul Ramchandani for his input in the design of this study, the Cambridge Mental Health in Schools Advisory Group for sharing their views and advice throughout the study, and the staff at the 6 schools that took part in this study for their time and effort. This study was funded by the UK Research and Innovation Emerging Minds network (grant ES/S004726/2), and the training was provided to the schools free of cost by Kognito. ES was funded by a Gates Cambridge Scholarship (grant OPP1144) for the duration of the study. MF is funded by the National Institute for Health and Care Research (NIHR) Oxford and Thames Valley Applied Research Collaboration at the Oxford Health National Health Service (NHS) Foundation Trust. PBJ is funded by the NIHR (grant 0616-20003). All research in the Cambridge Department of Psychiatry is supported by the NIHR Applied Research Collaboration East of England and the Cambridge Biomedical Research Centre at the Cambridgeshire and Peterborough NHS Foundation Trust. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, the Department of Health and Social Care, or the Bill & Melinda Gates Foundation.
Data Availability
The data sets generated during and analyzed during this study are not publicly available due to restrictions associated with our ethics approvals but are available from the corresponding author on reasonable request.
Conflicts of Interest
Kognito is a for-profit company. After reviewing their questionnaires on preparedness and self-efficacy and having found them rigorous and unbiased, we independently decided to include them as outcomes in our study. Kognito had no role in the study design, analysis, or publication. PBJ was a scientific advisory board member for MSD. All other authors declare no other conflicts of interest.
Teacher and Teaching Assistant Identification Form.
Kognito pre- and posttraining surveys.
Interview topic guides.
School characteristics.
Results from complete case sensitivity analysis.
Results from the sensitivity analysis excluding school D.
Quantitative and qualitative findings pertaining to the potential harms of At-Risk.
- Transforming children and young people's mental health provision: a green paper. Department of Health and Department for Education, United Kingdom Government. Dec 2017. URL: https://assets.publishing.service.gov.uk/media/5a823518e5 274a2e87dc1b56/Transforming_children_and_young_people_s_mental_health_provision.pdf [accessed 2024-03-25]
- Future in mind: promoting, protecting and improving our children and young people’s mental health and wellbeing. National Health Service England. URL: https://assets.publishing.service.gov.uk/media/5a80b26bed915d74e33fbe3c/Childrens_Mental _Health.pdf [accessed 2024-03-25]
- Promoting children and young people's mental health and wellbeing. Office for Health Improvement and Disparities and Department for Education, United Kingdom Government. Mar 20, 2015. URL: https://www.gov.uk/government/publications/promoting-children-and-young-peoples-emotional-health-and-wellbeing [accessed 2024-03-25]
- Newlove-Delgado T, Williams T, Robertson K, McManus S, Sadler K, Vizard T, et al. Mental health of children and young people in England 2021 - wave 2 follow up to the 2017 survey. National Health Service Digital. 2021. URL: https://openac cess.city.ac.uk/id/eprint/28718/ [accessed 2024-03-25]
- Vizard T, Sadler K, Ford T, Newlove-Delgado T, McManus S, Marcheselli F, et al. Mental health of children and young people in England, 2020. National Health Service Digital. Oct 22, 2020. URL: https://www.infocoponline.es/pdf/mhcyp _2020_rep.pdf [accessed 2024-03-25]
- Pitchforth J, Fahy K, Ford T, Wolpert M, Viner RM, Hargreaves DS. Mental health and well-being trends among children and young people in the UK, 1995-2014: analysis of repeated cross-sectional national health surveys. Psychol Med. Jun 2019;49(8):1275-1285. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Newlove-Delgado T, McManus S, Sadler K, Thandi S, Vizard T, Cartwright C, et al. Child mental health in England before and during the COVID-19 lockdown. Lancet Psychiatry. May 2021;8(5):353-354. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Creswell C, Shum A, Pearcey S, Skripkauskaite S, Patalay P, Waite P. Young people's mental health during the COVID-19 pandemic. Lancet Child Adolesc Health. Aug 2021;5(8):535-537. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Fazel M, Hoagwood K, Stephan S, Ford T. Mental health interventions in schools 1: mental health interventions in schools in high-income countries. Lancet Psychiatry. Oct 2014;1(5):377-387. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. Jun 2005;62(6):593-602. [ CrossRef ] [ Medline ]
- Greenberg MT, Domitrovich CE, Weissberg RP, Durlak JA. Social and emotional learning as a public health approach to education. Future Child. 2017;27(1):13-32. [ CrossRef ]
- Humphrey N, Wigelsworth M. Making the case for universal school-based mental health screening. Emot Behav Difficulties. 2016;21(1):22-42. [ CrossRef ]
- Kutcher S, Wei Y. School mental health: a necessary component of youth mental health policy and plans. World Psychiatry. Jun 2020;19(2):174-175. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Fazel M, Soneson E. Current evidence and opportunities in child and adolescent public mental health: a research review. J Child Psychol Psychiatry. Dec 2023;64(12):1699-1719. [ CrossRef ] [ Medline ]
- Stephan SH, Weist M, Kataoka S, Adelsheim S, Mills C. Transformation of children's mental health services: the role of school mental health. Psychiatr Res. Oct 2007;58(10):1330-1338. [ CrossRef ]
- Day L, Blades R, Spence C, Ronicle J. Mental health services and schools link pilots: evaluation brief. Department for Education, United Kingdom Government. Feb 2017. URL: https://assets.publishing.service.gov.uk/media/5a817dfaed915d74 e33fe812/Evaluation_of_the_MH_services_and_schools_link_pilots-RB.pdf [accessed 2024-03-25]
- Long MW, Albright G, McMillan J, Shockley KM, Price OA. Enhancing educator engagement in school mental health care through digital simulation professional development. J Sch Health. Sep 2018;88(9):651-659. [ CrossRef ] [ Medline ]
- Rothì DM, Leavey G, Best R. On the front-line: teachers as active observers of pupils’ mental health. Teach Teach Educ. Jul 2008;24(5):1217-1231. [ CrossRef ]
- Mazzer KR, Rickwood DJ. Teachers' role breadth and perceived efficacy in supporting student mental health. Adv Sch Ment Health Promot. 2015;8(1):29-41. [ CrossRef ]
- Shelemy L, Harvey K, Waite P. Supporting students’ mental health in schools: what do teachers want and need? Emot Behav Difficulties. 2019;24(1):100-116. [ CrossRef ]
- Fazel M, Soneson E, Sellars E, Butler G, Stein A. Partnerships at the interface of education and mental health services: the utilisation and acceptability of the provision of specialist liaison and teacher skills training. Int J Environ Res Public Health. Feb 24, 2023;20(5):4066. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Marshall L, Wishart R, Dunatchik A, Smith N. Supporting mental health in schools and colleges: quantitative survey. Department for Education, United Kingdom Government. Aug 2017. URL: https://assets.publishing.service.gov.uk/media/5a82e5bb40f0b6230269d46c/Supporting_Mental-Health_survey_report.pdf [accessed 2024-03-25]
- Sharpe H, Ford T, Lereya ST, Owen C, Viner RM, Wolpert M. Survey of schools' work with child and adolescent mental health across England: a system in need of support. Child Adolesc Ment Health. Sep 2016;21(3):148-153. [ CrossRef ] [ Medline ]
- Danby G, Hamilton P. Addressing the ‘elephant in the room’. The role of the primary school practitioner in supporting children’s mental well-being. Pastor Care Educ. 2016;34(2):90-103. [ CrossRef ]
- Reinke WM, Stormont M, Herman KC, Puri R, Goel N. Supporting children's mental health in schools: teacher perceptions of needs, roles, and barriers. Sch Psychol Q. 2011;26(1):1-13. [ CrossRef ]
- Kidger J, Gunnell D, Biddle L, Campbell R, Donovan J. Part and parcel of teaching? Secondary school staff's views on supporting student emotional health and well-being. Br Educ Res J. Jan 02, 2013;36(6):919-935. [ CrossRef ]
- Soneson E, Burn AM, Anderson JK, Humphrey A, Jones PB, Fazel M, et al. Determining stakeholder priorities and core components for school-based identification of mental health difficulties: a Delphi study. J Sch Psychol. Apr 2022;91:209-227. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Soneson E, Howarth E, Ford T, Humphrey A, Jones PB, Thompson Coon J, et al. Feasibility of school-based identification of children and adolescents experiencing, or at-risk of developing, mental health difficulties: a systematic review. Prev Sci. Jul 2020;21(5):581-603. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Childs-Fegredo J, Burn AM, Duschinsky R, Humphrey A, Ford T, Jones PB, et al. Acceptability and feasibility of early identification of mental health difficulties in primary schools: a qualitative exploration of UK school staff and parents’ perceptions. Sch Ment Health. Nov 18, 2020;13:143-159. [ CrossRef ]
- Anderson JK, Ford T, Soneson E, Coon JT, Humphrey A, Rogers M, et al. A systematic review of effectiveness and cost-effectiveness of school-based identification of children and young people at risk of, or currently experiencing mental health difficulties. Psychol Med. Sep 13, 2018;49(1):9-19. [ CrossRef ]
- Yamaguchi S, Foo JC, Nishida A, Ogawa S, Togo F, Sasaki T. Mental health literacy programs for school teachers: a systematic review and narrative synthesis. Early Interv Psychiatry. Feb 2020;14(1):14-25. [ CrossRef ] [ Medline ]
- Kognito homepage. Kognito. URL: https://kognito.com/ [accessed 2024-03-26]
- At-risk for elementary school educators. Kognito. URL: https://kognito.com/products/at-risk-for-elementary-schools [accessed 2024-03-25]
- Anderson M, Werner-Seidler A, King C, Gayed A, Harvey SB, O’Dea B. Mental health training programs for secondary school teachers: a systematic review. Sch Ment Health. Oct 3, 2018;11:489-508. [ CrossRef ]
- Ekornes S. Teacher perspectives on their role and the challenges of inter-professional collaboration in mental health promotion. Sch Ment Health. Mar 17, 2015;7:193-211. [ CrossRef ]
- Ohrt JH, Deaton JD, Linich K, Guest JD, Wymer B, Sandonato B. Teacher training in K–12 student mental health: a systematic review. Psychol Sch. Mar 03, 2020;57(5):833-846. [ CrossRef ]
- Parker BL, Anderson M, Batterham PJ, Gayed A, Subotic-Kerry M, Achilles MR, et al. Examining the preliminary effectiveness and acceptability of a web-based training program for Australian secondary school teachers: pilot study of the BEAM (building educators' skills in adolescent mental health) program. JMIR Ment Health. Oct 22, 2021;8(10):e29989. [ FREE Full text ] [ CrossRef ] [ Medline ]
- McVey G, Gusella J, Tweed S, Ferrari M. A controlled evaluation of web-based training for teachers and public health practitioners on the prevention of eating disorders. Eat Disord. 2009;17(1):1-26. [ CrossRef ] [ Medline ]
- Pereira CA, Wen CL, Miguel EC, Polanczyk GV. A randomised controlled trial of a web-based educational program in child mental health for schoolteachers. Eur Child Adolesc Psychiatry. Aug 2015;24(8):931-940. [ CrossRef ] [ Medline ]
- Kognito At-Risk in PK-12. Oklahoma Department of Mental Health and Substance Abuse Services. URL: https://oklahoma.gov/odmhsas/trainings/training-institute/at-risk-pk-12.html [accessed 2024-03-14]
- Albright G, Fazel M, Khalid N, McMillan J, Hilty D, Shockley K, et al. High school educator training by simulation to address emotional and behavioral concerns in school settings: a randomized study. J Technol Behav Sci. 2022;7(3):277-289. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Greif Green J, Levine RS, Oblath R, Corriveau KH, Holt MK, Albright G. Pilot evaluation of preservice teacher training to improve preparedness and confidence to address student mental health. Evid Based Pract Child Adolesc Ment Health. 2020;5(1):42-52. [ CrossRef ]
- Domitrovich CE, Bradshaw CP, Poduska JM, Hoagwood K, Buckley JA, Olin S, et al. Maximizing the implementation quality of evidence-based preventive interventions in schools: a conceptual framework. Adv Sch Ment Health Promot. Jul 2008;1(3):6-28. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Bonell C, Prost A, Melendez-Torres GJ, Davey C, Hargreaves JR. Will it work here? A realist approach to local decisions about implementing interventions evaluated as effective elsewhere. J Epidemiol Community Health. Jan 2021;75(1):46-50. [ CrossRef ] [ Medline ]
- Domitrovich CE, Greenberg MT. The study of implementation: current findings from effective programs that prevent mental disorders in school-aged children. J Educ Psychol Consult. 2000;11(2):193-221. [ CrossRef ]
- Evans RE, Craig P, Hoddinott P, Littlecott H, Moore L, Murphy S, et al. When and how do 'effective' interventions need to be adapted and/or re-evaluated in new contexts? The need for guidance. J Epidemiol Community Health. Jun 2019;73(6):481-482. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Gardner F, Montgomery P, Knerr W. Transporting evidence-based parenting programs for child problem behavior (age 3-10) between countries: systematic review and meta-analysis. J Clin Child Adolesc Psychol. 2016;45(6):749-762. [ CrossRef ] [ Medline ]
- Leijten P, Melendez-Torres GJ, Knerr W, Gardner F. Transported versus homegrown parenting interventions for reducing disruptive child behavior: a multilevel meta-regression study. J Am Acad Child Adolesc Psychiatry. Jul 2016;55(7):610-617. [ CrossRef ] [ Medline ]
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new medical research Council guidance. BMJ. Sep 29, 2008;337:a1655. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Moore L, Hallingberg B, Wight D, Turley R, Segrott J, Craig P, et al. Exploratory studies to inform full-scale evaluations of complex public health interventions: the need for guidance. J Epidemiol Community Health. Oct 2018;72(10):865-866. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Eldridge SM, Lancaster GA, Campbell MJ, Thabane L, Hopewell S, Coleman CL, et al. Defining feasibility and pilot studies in preparation for randomised controlled trials: development of a conceptual framework. PLoS One. 2016;11(3):e0150205. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Bowen DJ, Kreuter M, Spring B, Cofta-Woerpel L, Linnan L, Weiner D, et al. How we design feasibility studies. Am J Prev Med. May 2009;36(5):452-457. [ FREE Full text ] [ CrossRef ] [ Medline ]
- McLennan D, Noble S, Noble M, Plunkett E, Wright G, Gutacker N. The English indices of deprivation 2019: technical report. Ministry of Housing, Communities and Local Government, United Kingdom Government. Sep 2019. URL: https://dera.ioe.ac.uk/34259/1/IoD2019_Technical_Report.pdf [accessed 2024-03-25]
- Schools, pupils and their characteristics: January 2019. Department for Education, United Kingdom Government. Jun 2019. URL: https://www.gov.uk/government/statistics/schools-pupils-and-their-characteristics-january-2019 [accessed 2024-03-25]
- Special educational needs in England: January 2019. Department for Education, United Kingdom Government. Jul 4, 2019. URL: https://assets.publishing.service.gov.uk/media/5d1c91cce5274a08df3d35bd/SEN_2019_Text.docx.pdf [accessed 2024-03-25]
- Goodman R. The Strengths and Difficulties Questionnaire: a research note. J Child Psychol Psychiatry. Jul 07, 1997;38(5):581-586. [ CrossRef ] [ Medline ]
- Goodman R. The extended version of the Strengths and Difficulties Questionnaire as a guide to child psychiatric caseness and consequent burden. J Child Psychol Psychiatry. Jul 1999;40(5):791-799. [ CrossRef ]
- Goodman R, Ford T, Simmons H, Gatward R, Meltzer H. Using the Strengths and Difficulties Questionnaire (SDQ) to screen for child psychiatric disorders in a community sample. Br J Psychiatry. Dec 02, 2000;177(6):534-539. [ CrossRef ] [ Medline ]
- Goodman R, Meltzer H, Bailey V. The Strengths and Difficulties Questionnaire: a pilot study on the validity of the self-report version. Eur Child Adolesc Psychiatry. Sep 12, 1998;7(3):125-130. [ CrossRef ] [ Medline ]
- Stone LL, Otten R, Engels RC, Vermulst AA, Janssens JM. Psychometric properties of the parent and teacher versions of the Strengths and Difficulties Questionnaire for 4- to 12-year-olds: a review. Clin Child Fam Psychol Rev. Sep 2010;13(3):254-274. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Albright GL, Davidson J, Goldman R, Shockley KM, Timmons-Mitchell J. Development and validation of the Gatekeeper Behavior Scale. Crisis. Jul 2016;37(4):271-280. [ CrossRef ] [ Medline ]
- Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. Aug 07, 2009;4:50. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Lyon AR, Bruns EJ. From evidence to impact: joining our best school mental health practices with our best implementation strategies. School Ment Health. Mar 1, 2019;11(1):106-114. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Schools, pupils and their characteristics: January 2020. Department for Education, United Kingdom Government. Jun 25, 2020. URL: https://www.gov.uk/government/statistics/schools-pupils-and-their-characteristics-january-2020 [accessed 2024-03-25]
- Eldridge SM, Chan CL, Campbell MJ, Bond CM, Hopewell S, Thabane L, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. Oct 24, 2016;355:i5239. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Wilson DT, Walwyn RE, Brown J, Farrin AJ, Brown SR. Statistical challenges in assessing potential efficacy of complex interventions in pilot or feasibility studies. Stat Methods Med Res. Jun 2016;25(3):997-1009. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Lancaster GA, Dodd S, Williamson PR. Design and analysis of pilot studies: recommendations for good practice. J Eval Clin Pract. May 2004;10(2):307-312. [ CrossRef ] [ Medline ]
- Thabane L, Ma J, Chu R, Cheng J, Ismaila A, Rios LP, et al. A tutorial on pilot studies: the what, why and how. BMC Med Res Methodol. Jan 06, 2010;10:1. [ FREE Full text ] [ CrossRef ] [ Medline ]
- R: a language and environment for statistical computing. The Comprehensive R Archive Network. Feb 10, 2015. URL: https://www.gbif.org/tool/81287/r-a-language-and-environment-for-statistical-computing [accessed 2024-03-25]
- Wickham H. Ggplot2: Elegant Graphics for Data Analysis. New York, NY. Springer; 2009.
- Bryer J, Speerschneider K. Analysis and visualization of Likert based items. GitHub. URL: http://github.com/jbryer/likert
- YouthinMind homepage. YouthinMind. URL: https://youthinmind.com/ [accessed 2024-03-26]
- Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. Nov 2005;15(9):1277-1288. [ CrossRef ] [ Medline ]
- Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. Sep 18, 2013;13:117. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77-101. [ CrossRef ]
- Braun V, Clarke V. Thematic Analysis: A Practical Guide. Thousand Oaks, CA. SAGE Publications; 2021.
- School workforce in England. United Kingdom Government. Jun 8, 2023. URL: https://explore-education-statistics.service .gov.uk/find-statistics/school-workforce-in-england [accessed 2024-03-14]
- Jorm AF, Kitchener BA, Sawyer MG, Scales H, Cvetkovski S. Mental health first aid training for high school teachers: a cluster randomized trial. BMC Psychiatry. Jun 24, 2010;10:51. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Moor S, Maguire A, McQueen H, Wells EJ, Elton R, Wrate R, et al. Improving the recognition of depression in adolescence: can we teach the teachers? J Adolesc. Feb 2007;30(1):81-95. [ CrossRef ] [ Medline ]
- Kidger J, Stone T, Tilling K, Brockman R, Campbell R, Ford T, et al. A pilot cluster randomised controlled trial of a support and training intervention to improve the mental health of secondary school teachers and students - the WISE (Wellbeing in Secondary Education) study. BMC Public Health. Oct 06, 2016;16(1):1060. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Vieira MA, Gadelha AA, Moriyama TS, Bressan RA, Bordin IA. Evaluating the effectiveness of a training program that builds teachers' capability to identify and appropriately refer middle and high school students with mental health problems in Brazil: an exploratory study. BMC Public Health. Feb 28, 2014;14:210. [ FREE Full text ] [ CrossRef ] [ Medline ]
- McLaughlin RJ, Holcomb JD, Jibaja-Rusth ML, Webb J. Teacher ratings of student risk for substance use as a function of specialized training. J Drug Educ. 1993;23(1):83-95. [ CrossRef ]
- Soneson E, Childs-Fegredo J, Anderson JK, Stochl J, Fazel M, Ford T, et al. Acceptability of screening for mental health difficulties in primary schools: a survey of UK parents. BMC Public Health. Dec 22, 2018;18(1):1404. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Levitt JM, Saka N, Hunter Romanelli L, Hoagwood K. Early identification of mental health problems in schools: the status of instrumentation. J Sch Psychol. Apr 2007;45(2):163-191. [ CrossRef ]
- Loades ME, Mastroyannopoulou K. Teachers' recognition of children's mental health problems. Child Adolesc Ment Health. Sep 2010;15(3):150-156. [ CrossRef ] [ Medline ]
- Anderson JK, Howarth E, Vainre M, Jones PB, Humphrey A. A scoping literature review of service-level barriers for access and engagement with mental health services for children and young people. Child Youth Serv Rev. Jun 2017;77:164-176. [ CrossRef ]
- Moon J, Williford A, Mendenhall A. Educators' perceptions of youth mental health: implications for training and the promotion of mental health services in schools. Child Youth Serv Rev. Feb 2017;73:384-391. [ CrossRef ]
- Graham A, Phelps R, Maddison C, Fitzgerald R. Supporting children’s mental health in schools: teacher views. Teach Teach. 2011;17(4):479-496. [ CrossRef ]
- Atkins MS, Graczyk PA, Frazier SL, Abdul-Adil J. Toward a new model for promoting urban children's mental health: accessible, effective, and sustainable school-based mental health services. Sch Psychol Rev. 2003;32(4):503-514. [ CrossRef ]
- Moore A, Stapley E, Hayes D, Town R, Deighton J. Barriers and facilitators to sustaining school-based mental health and wellbeing interventions: a systematic review. Int J Environ Res Public Health. Mar 17, 2022;19(6):3587. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Gee B, Wilson J, Clarke T, Farthing S, Carroll B, Jackson C, et al. Review: delivering mental health support within schools and colleges - a thematic synthesis of barriers and facilitators to implementation of indicated psychological interventions for adolescents. Child Adolesc Ment Health. Feb 2021;26(1):34-46. [ CrossRef ] [ Medline ]
- Fält E, Wallby T, Sarkadi A, Salari R, Fabian H. Agreement between mothers', fathers', and teachers' ratings of behavioural and emotional problems in 3-5-year-old children. PLoS One. Nov 01, 2018;13(11):e0206752. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Bear HA, Ayala Nunes L, DeJesus J, Liverpool S, Moltrecht B, Neelakantan L, et al. Determination of markers of successful implementation of mental health apps for young people: systematic review. J Med Internet Res. Nov 09, 2022;24(11):e40347. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Durbin K, Harmon S. We are on the same team: child psychiatry and the school system. JAACAP Connect. 2020;7(1):32-36. [ CrossRef ]
Abbreviations
Edited by T Leung; submitted 24.02.23; peer-reviewed by E Widnall, B Fernandes, J Burns, K Cohen; comments to author 27.08.23; accepted 01.03.24; published 23.04.24.
©Emma Soneson, Emma Howarth, Alison Weir, Peter B Jones, Mina Fazel. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 23.04.2024.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in the Journal of Medical Internet Research, is properly cited. The complete bibliographic information, a link to the original publication on https://www.jmir.org/, as well as this copyright and license information must be included.
IMAGES
VIDEO
COMMENTS
In this course you will be introduced to the basic ideas behind the qualitative research in social science. You will learn about data collection, description, analysis and interpretation in qualitative research. Qualitative research often involves an iterative process. We will focus on the ingredients required for this process: data collection ...
In summary, here are 10 of our most popular qualitative research methods courses. Qualitative Research Methods: University of Amsterdam. Qualitative Research Design and Methods for Public Health: Emory University. Understanding Research Methods: University of London. Qualitative Research: University of California, Davis.
Best online courses in Qualitative Research from MIT, University of Michigan, Yale, University of Illinois and other top universities around the world ... Learn about qualitative research methods, data analysis, and the strengths and challenges of various research techniques. Add to list YouTube 8 hours On-Demand Free Online Course ...
This course provides an applied, phenomenological approach to qualitative data analysis. It is designed for an interdisciplinary audience with examples taken from the nonprofit, commercial, and government sectors in the health and social sciences. Undergraduate/graduate students, research staff, and IRB members in particular may find this ...
The University of Oxford's expert-led programme of short courses in qualitative research methods aims to equip participants with the knowledge and skills to design, conduct, and interpret qualitative research. ... meta-ethnography, and qualitative data analysis. This highly-regarded programme is delivered in online and face-to-face formats to ...
This two-day online course introduces the principles and practice of qualitative data analysis, with emphasis on thematic analysis. Over two days our approachable and research-active experts will show that analysis is achievable though an accessible step-by-step process, and will provide de-identified data for you to work with.
In this course you will learn about the foundations of qualitative inquiry—and how it differs from quantitative research. You will gain practice in common qualitative traditions—like phenomenology and ethnography—and some of the methods they use, such as interviewing. You will gain the competence, confidence, and "know-how" to begin planning your very own qualitative study of a topic ...
1700 Coursera Courses That Are Still Completely Free. In this course you will be introduced to the basic ideas behind the qualitative research in social science. You will learn about data collection, description, analysis and interpretation in qualitative research. Qualitative research often involves an iterative process.
The Odum Institute has joined ResearchTalk, Inc., in presenting the Qualitative Research Summer Intensive, a five-day qualitative research professional development course series, offered annually in July. The intensive includes courses on qualitative traditions, research design, data collection, analysis, and innovative strategies in the field.
The first half of the course is covered in 21A.819.1x, and covers an introduction to qualitative research and conducting interviews. This course consists of the second half of the course, and covers what to do with the data once you have started collecting it. This will include transcribing data, creating codes and codebooks, coding data ...
A course providing an introduction to qualitative research methods in education. EDCI 61600: Qualitative Data Collection and Analysis in Educational Research (3 cr.) A course focused on collection and analysis of qualitative data; Elective #1: with focus on qualitative methods (3 cr.) Elective #2: with focus on qualitative methods (3 cr.)
This course is designed as a basic introduction to the complex world of research methods and provides both theoretical and practical information for students to give them a foundation for carrying out research in a wide range of disciplines using quantitative, qualitative, and mixed methods. 8 weeks. 1-2 hours per week.
Get an introduction to what qualitative research is, the types of qualitative research methods, the appropriate situations to apply qualitative methods, and how to conduct your own qualitative research. You learn to build a research protocol and use various techniques to design, conduct, analyze and present an informative research study. > <p>At the end of the course, you are expected to ...
This course presents a detailed overview of qualitative methods of data collection, including observation, interviews, and focus group discussions. ... This course will introduce you to MAXQDA software for easier data analysis during the qualitative research process. You'll explore how to do memos, variables, segmentation, coding, and data ...
Course Description This course will focus on approaches to the analysis of qualitative data. It is designed for students who have some experience with qualitative field research methods (introductory coursework or project experience) and have a set of qualitative data they are interested in analyzing for their own research.
This course aims to equip you with the knowledge and skills to understand, design and conduct high quality qualitative research. The course will help you: gain a clear understanding of the principles of qualitative research; practise skills including interviewing, running a focus group, data analysis, and developing and presenting a research ...
Qualitative research is the opposite of quantitative research, which involves collecting and analyzing numerical data for statistical analysis. Qualitative research is commonly used in the humanities and social sciences, in subjects such as anthropology, sociology, education, health sciences, history, etc. Qualitative research question examples
Who this course is for: Those willing to learn to use NVivo for Qualitative data analysis (Beginner Level) Those who have already used this software but want to develop their skills further (Pre-intermediate Level) Students undertaking their Master's/PhD study. Academics & Researchers wishing to improve their skill set.
This live online course explores the use of narratives and storytelling in qualitative research. * Price: £165 for SRA members, £220 for non-members. It runs in one day and uses Zoom software * Read More. ... This live online course provides qualitative data analysis techniques using narrative analysis. (Advanced level) * Price: £165 for SRA ...
But don't worry! Qualitative analysis can be rewarding and fun. In this free qualitative research course, we'll show you how to overcome these challenges by teaching you the basics of qualitative coding methods. This process has helped many students and researchers finish their dissertations and research on time.
comprehensive training in research methods. NCRM delivers training and resources at core and advanced levels, covering quantitative, qualitative, digital, creative, visual, mixed and multimodal methods. 20th Anniversary Impact Prize. Tell us how NCRM has helped you to make an impact ...
Five Basic Approaches to Qualitative Research • 4 minutes. Qualitative and Quantitative As Complementary Methods • 3 minutes. 4 readings • Total 145 minutes. Course Outline and Grading Information • 5 minutes. Introduction to Qualitative Research • 20 minutes. Qualitative Inquiry • 90 minutes.
Introduction to Data Analytics. About: This course offers an introduction to data analysis, the role of a data analyst, and the various tools used for data analytics. This course is offered by IBM ...
Design. The research was designed using a descriptive phenomenological pattern, one of the qualitative research methods. Phenomenology offers a diverse range of qualitative research methods for healthcare, allowing for a deeper understanding of human experiences and their impact on healthcare systems (Rodriguez & Smith, 2018).Phenomenological research was preferred for this research because it ...
Study design. This qualitative explorative research helped the researcher facilitate data collection, analysis, and interpretation of the finding processes [].The approach enabled an unrestrained process that explored the participants' information needs regarding the care of children with ID in a rural home environment.
The qualitative findings indicated that school staff perceived the training as useful, practical, and acceptable. ... outcomes across time points by comparing medians and IQRs and analyzed qualitative data using reflexive thematic analysis. Results: A total of 108 teachers and teaching assistants (TAs) completed T1 questionnaires, 89 (82.4% ...